1701006002 CASE PRESENTATION
LONG CASE
CASE DISCUSSION:
A 40 years old Male, resident of bhongir, painter by occupation presented to OPD with chief complaints of
- Shortness of breath since 7 days
- Chest Pain on left side since 5days
Patient was apparently asymptomatic 7days back then developed shortness of breath which was
- insidious in onset
- gradually progressive (grade I to grade II according to MMRC)
- Chest pain:
non radiating
nature: pricking type - loss of weight(about 10kgs in past 1yr)
- loss of appetite
- Vomitings
- Orthopnea, PND
- Edema
- palpitations
- Wheeze
- chest tightness
- cough
- hemoptysis
- Diabetes Mellitus 3 yrs back (on medication- Metformin 500mg, Glimiperide 1mg)
- Mixed diet
- sleep is adequate ( but disturbed from past few days)
- loss of appetite is present
- bowel and bladder movements are regular
- He used to Consume
Alcohol stopped 20years back ( 90ml per day)
Smoking from past 20years (10 cigarettes per day) but stopped 2years back.
Pulse rate : 139beats/min
BP : 110/70 mm Hg
RR : 45 cpm
SpO2 : 91% at room air
GRBS : 201mg/dl



- RESPIRATORY EXAMINATION:
INSPECTION:
Shape of chest is elliptical,
B/L asymmetrical chest,
Trachea in central position,
Expansion of chest- Right- normal, left-decreased,
Use of Accessory muscles is present.
PALPATION:
All inspectory findings are confirmed,
No tenderness, No local rise of temperature,
trachea is deviated to the right,
Measurement:
AP: 24cm
Transverse:28cm
Right hemithorax:42cm
left hemithorax:40cm
Circumferential:82cm
Tactile vocal fremitus: decreased on left side ISA, InfraSA, AA, IAA.
PERCUSSION: Stony dull note present in left side ISA, InfraSA, AA, IAA.
AUSCULTATION:
B/L air entry present, vesicular breath sounds heard,
Decreased intensity of breath sounds in left SSA,IAA,
Absent breath sounds in left ISA.
- CVS EXAMINATION:
S1,S2 heard
No murmurs. No palpable heart sounds.
JVP: normal
Apex beat: normal - PER ABDOMEN:
Soft, Non-tender
No organomegaly
Bowel sounds heard
no guarding/rigidity - CNS EXAMINATION:
No focal neurological deficits
Gait- NORMAL
Reflexes: normal
DB: 0.74mg/dl
AST: 24IU/L
ALT: 09IU/L
ALP: 167IU/L
TP: 7.5gm/dl
ALB: 3.29gm/dl

INTERPRETATION: As 2 values are greater than the normal we consider as an EXUDATIVE EFFUSION.
(confirmation after pleural fluid c/s analysis)




- O2 inhalation with nasal prongs with 2-4 lt/min to maintain SPO2 >94%
- Inj. Augmentin 1.2gm/iv/TID
- Inj. Pan 40mg/iv/OD
- Tab. Pcm 650mg/iv/OD
- Syp. Ascoril-2tsp/TID
- DM medication taken regularly
- High Protein diet
- 2 egg whites/day
- Monitor vitals
- GRBS every 6th hourly
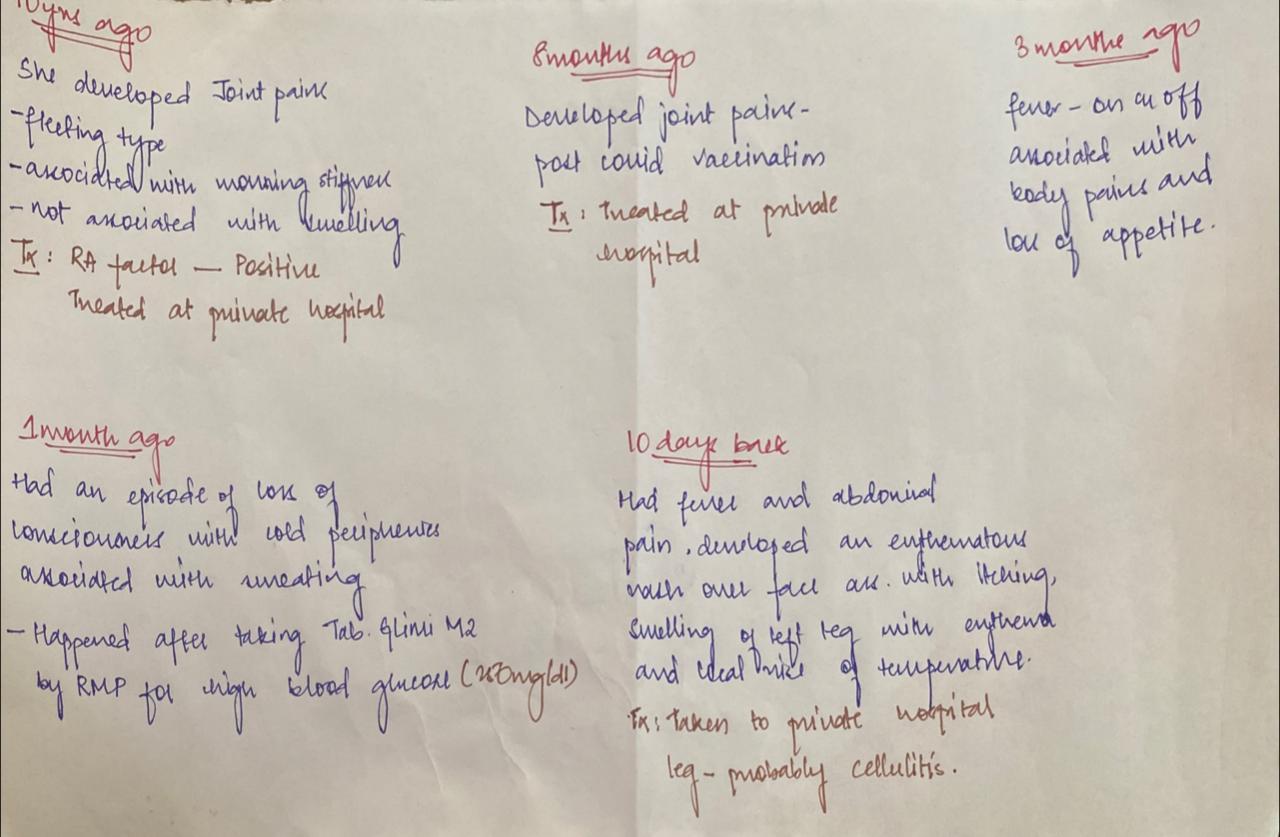
A 45 year old lady, resident of Nalgonda, Tailor by occupation presented to GM OPD with chief complaints of
- Fever since 3months
- Body pains since 3months
- loss of appetite since 3months
- Appearance of facial rash since 10days
CLINICAL IMAGES:




.jpeg)
Patient had a history of diminution of vision which started at the age of 15 years.
For which she was advised use of
- To use spectacles
No h/o any trauma,
Not a known case of DM/HTN/ASTHMA/CAD /EPILEPSY/TB
PERSONAL HISTORY:
Diet- mixed
Appetite- decreased
Bowel and bladder- regular
Sleep- disturbed
Addictions- nil
FAMILY HISTORY:
No similar complaints in the family.
GENERAL EXAMINATION :
Pallor present
no signs of edema, icterus, clubbing, cyanosis, lymphadenopathy.
VITALS:
Pulse rate : 72beats/min
BP : 110/70 mm Hg
RR : 18 cpm
SpO2 : 98% at room air
SYSTEMIC EXAMINATION:
CVS:
INSPECTION: shows no scars on the chest, no features of raised JVP, no additional visible pulsations seen.
PALPATION: all inspectory findings are confirmed, apex beat normal at 5th ics medial to mcl, no additional palpable pulsations or murmurs
PERCUSSION: showed normal heart borders
AUSCULTATION:S1 S2 heard no murmurs or additional sounds
CNS:
C/C/C
MOTOR-: normal tone and power
reflexes: RT LT
BICEPS ++ ++
TRICEPS ++ ++
SUPINATOR ++ ++
KNEE ++ ++
SENSORY : touch, pressure, vibration, and proprioception are normal in all limbs.
GIT:
INSPECTION: normal scaphoid abdomen with no pulsations and scars
PALPATION: all inspectory findings are confirmed, no organomegaly, non tender and soft PERCUSSION: normal resonant note present, liver border normal
AUSCULTATION: normal abdominal sounds heard, no bruit present.
RESPIRATORY:
INSPECTION: normal chest shape bilaterally symmetrical, mediastinum central
no scars, Rr normal, no pulsations
PALPATION: Insp findings are confirmed
PERCUSSION: normal resonant note present bilaterally
AUSCULTATION: B/L air entry present, vesicular breath sounds heard.
PROVISIONAL DIAGNOSIS:
? Secondary sjogren syndrome
Anemia
INVESTIGATIONS:
RBS: 136mg/dl
HEMOGRAM:
HB: 6.9
TC: 9700
MCV: 85.1
PCV: 21.7
MCH: 27.1
MCHC: 31.8
PLT: 1.57
ESR: 90
SMEAR: ANISOCYTOSIS
RFT:
Blood Urea: 20mg/dl
S. Creatinine: 1.1mg/dl
Na: 136
K: 3.3
Cl: 98
LFT:
TB: 0.45
DB: 0.17
AST: 60
ALT: 17
ALP: 138
TP: 6.3
ALB: 2.18
CUE:
ALB +
Sugars nil
Pus cells nil
ESR - 90
CRP - NEGETIVE
HCV: NEGETIVE
HBV: NEGETIVE
HIV: NEGETIVE

TREATMENT:
- Tab. Pan 40mg/PO/OD
- Tab. Deflazocort 6mg/PO/BD
- Tab. cefixime 200mg/PO/BD
- Tab. Orofex-XT (15 mins before food)/PO/OD
- Tab. Teczine 10mg/PO/OD
- Hydrocortisone cream 1%/LA/OD for 1 week (on face).
- GRBS every 6th hourly
- Monitor vitals.



Comments
Post a Comment