1701006059 CASE PRESENTATION
LONG CASE
A 46 year old male came to casuality with chief complaints of :
-burning micturition since 10days
-vomiting since 2days (3-4 episodes)
-giddiness since 1day
History of presenting illness:
Patient was apparently asymptomatic 10 days back then he developed burning micturition, vomiting since 2 days containing food particles, non bilious,non foul smelling(3-4 episodes),later he complained of giddiness for which he was brought to our hospital and his GRBS was recorded high value for which he was given NPH 10U and HAI 10U.
No history of fever/cough/cold
No significant history of UTIs

Past history:
10years back patient complained of polyuria for which he was diagnosed with Type 2 Diabetes Mellitus, he was started on oral hypoglycemic agents(OHA) 10years back
3years back OHAs were converted into Insulin
3years back he underwent cataract surgery
1year back he had injury to his right leg, which gradually progressed to non healing ulcer extending upto below knee and ended with undergoing below knee amputation due to developement of wet gangrene.
Delayed wound healing was present- it took 2months to heal
Not a k/c/o Hypertension, Epilepsy,Tuberculosis, Thyroid
Not on any medication
No history of blood transfusion
Personal history:
Diet - Mixed
Appetite- normal
Sleep- Adequate
Bowel and bladder- Regular
Micturition- burning micturition present
Habits/Addiction:
Alcohol-
Not consuming alcohol since 1 yr.
Previously (1yr back) Regular consumption of alcohol, about 90mL whiskey consumed almost daily.Also 1 month on & off consumption pattern previously present
Family history:
Not significant
Vitals @ Admission:
BP: 110/80 mmHg
HR: 98 bpm
RR: 18 cpm
TEMP: 99F
SpO2: 98% on RA
GRBS: 124 mg/dL
General Examination:
Pallor present
No- icterus,cyanosis,clubbing,koilonychia, lymphadenopathy
No dehydration





Systemic Examination:
CVS: S1S2 heard, No murmurs
RS: BAE+,NVBS
P/A: Soft, Non tender
CNS:
Reflexes: (Biceps/Triceps/Knee/Ankle/Plantar)Normal
Power: Normal(5/5) in both Upper and Lower limbs
Tone: Normal in both Upper and Lower limbs
No meningeal signs
Investigations:
On admission (19.5.22)


X ray KUB

CT Scan

Liver function tests:

Renal function tests:

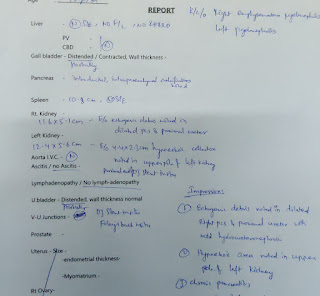
Ultrasound report abdomen and pelvis
 |
20.05.22
LDH- 192
24hr Urinary protein- 434
24hrs Urinary creatinine- 0.5
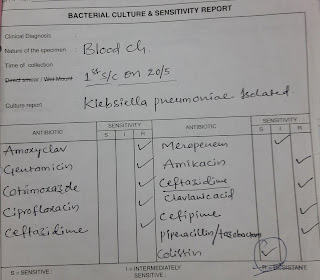
Culture report: Klebsiella Pneumonia positive


Pus cells
21.5.22
Hemoglobin- 6.8g%
TLC- 22,500cells/cumm
Platelets- 1.4lakhs/cu.mm
Urea- 155mg/dl
Creatinine- 4.7
Uric acid- 7.1
Phosphorus- 2.0
Sodium- 126
Potassium- 2.6
Chloride- 87
22.5.22
Hemoglobin- 7.2
TLC- 17,409
Platelet count- 1.5
Urea- 162
Uric acid- 5.0
Sodium- 125
Chloride- 88
23.2.22
25.5.22
27.5.22
Hb- 7
TLC- 22,000
Platelet count- 26,000
Urea- 144
Creatinine - 4.8
Uric acid-9.1
Phosphorus- 4.8
Sodium- 135
Potassium- 4.3
Chloride- 98
Fasting blood sugar- 149
29.5.22
Hb- 6.4
TLC- 14,700
Platelet count- 6000
Urea - 149
Creatinine- 4.4
Uric acid- 9.2
Provisional Diagnosis:
Right emphysematous pyelonephiritis and left acute pyelonephiritis and encephalopathy secondary to sepsis.
H/o of Type 2 Diabetes mellitus since 10years
Treatment:
Day 1 to Day 3:
INJ. MEROPENEM 500mg IV BD
INJ. ZOFER 4mg IV TID
INJ. PAN 40mg IV OD
IV Fluids- NS,RL @ 100 mL/hr
BP/HR/RR/SpO2 charting
Temp charting 4th hrly
RT feeds- 2nd hrly 100 mL water
Day 4
INJ. MEROPENEM 500mg IV BD
INJ. ZOFER 4mg IV TID
INJ. RANTAC 50mg IV OD
INJ. KCl 2 Amp in 500 mL NS over 4.5 hrs infusion
IV Fluids- NS,RL @ 100 mL/hr
SYP. POTCHLOR 10 mL in 1 glass of water TID
SYP. MUCAINE GEL 10 mL PO TID
7 point profile
BP/HR/RR/SpO2 charting
Temp charting 4th hrly
RT feeds- 2nd hrly 100 mL water
Day 5 to Day 10:
INJ. MEROPENEM 500mg IV BD (Day 6)
INJ. ZOFER 4mg IV TID
INJ. RANTAC 50mg IV OD
INJ. LASIX 40 mg IV BD
IV Fluids- NS,RL @ 100 mL/hr
SYP. MUCAINE GEL 10 mL PO TID
GRBS 7 point profile
INJ.HAI SC TID ACC to GRBS
TAB.DOLO 650 mg SOS
BP/HR/RR/SpO2 charting
Temp charting 4th hrly
Day 11:
INJ. COLISTIN 2.25 MU IV OD(Day 4)
INJ. ZOFER 4mg IV TID
INJ. RANTAC 50mg IV OD
INJ. LASIX 40 mg IV BD
IV Fluids- NS,RL @ 100 mL/hr
SYP. MUCAINE GEL 10 mL PO TID
GRBS 7 point profile
INJ.HAI SC TID ACC to GRBS
TAB.DOLO 650 mg SOS
Day 12:
SDP Transfusion done I/v/o low platelet count
Pre transfusion counts:
Hb:6.2 g/dL
TLC:14700
PLt:6000
Post transfusion counts:
Hb:6.4
TLC:13700
PLt:50000
------------------------------------------------------------------------------------------------------------------------------------
SHORT CASE
Abdominal Distension since 1 year
Facial puffiness since 1 year
Itching all over the body since 1 year and developed multiple plaques on abdomen and Lower limbs
pedal edema since 5 days pitting type
H/O PRESENT ILLNESS
Patient was apparently asymptomatic 1 year back then she developed abdominal distension, facial puffiness,itching all over the body and 5 days ago she developed pedal edema and SOB grade 3.
she had an episode of vomiting two days back which contained food particles. It was relieved on medication.
PAST HISTORY
she developed B/L Knee pain - since 3years, onset - insidious, gradually progressing, type- pricking, more at the night, aggravated on walking, relieved on sitting n sleeping, no radiation and is under medication( demisone 0.5 mg and acelogic SR)
She developed abdominal distension and facial puffiness one year back.
She also developed itching and skin lesions and was diagnosed as tinea and was given medications.
Not a K/C/O DM/HTN/ asthma / Ischemic heart disease / epilepsy / TB
FAMILY HISTORY
NO SIGNIFICANT FAMILY HISTORY
PERSONAL HISTORY:
OCCUPATION Daily wage worker , stopped going to work since 3 months
DIET MIXED
APPETITE decreased
SLEEP NORMAL
BOWEL AND BLADDER HABITS : decreased urine output
ADDICTIONS: NO
Patient is concious coherent and coperative, well oriented to time palce and person.
VITALS
BP 110/80
PR 90bpm
TEMP 98.5degrees F
SPO2 98 @ RA
GRBS 106
No Pallor , ICTERUS , CYANOSIS, CLUBBING , LYMPHADENOPATHY
Inspection:
Abdomen is distended
Umbilicus is inverted
Movements :- gentle rise in abdominal wall in inspiration and fall during expiration.
No visible gastric peristalsis
palpation : SOFT, NON TENDER, NO ORGANOMEGALY
RS - BAE + , normal vesicular breath sounds




Random Blood sugar

Renal function test

Liver function test

Complete blood picture

Lipid profile

Ultrasound:

X-ray


Provisional diagnosis : Steroid induced cushings syndrome
Treatment:
4-06-2022
Inj. Pantop
Inj lasix
Inj optineuron
Tab. Ultracet
Tab. Atarax
Tab . Zofer
Luliconazole
Syp aristozyme
5-06-2022
Ultracet
Luliconazole ointment
Rantac
Syp aristozyme
6-06-2022
Ultracet
Luliconazole ointment
Rantac
T defloz 6mg
Syp. Aristozyme
7-06-2022
Ultracet
Luliconazole ointment
Rantac
Syp. Aristozyme



{kind=link}
Comments
Post a Comment