1701006064 CASE PRESENTATION
LONG CASE
A 26 year old female from nalgonda who is a homemaker came to the hospital with the chief complaints of :
• Lower back pain since 15 days
• Fever since 10 days
History of presenting illness:
• The patient was apparently asymptomatic 15 days back, then she developed lower back pain which was insidious in onset and gradually progressive, and continuous dragging type which finally became severe pain. Pain is more during night time. The severity of pain is decreased after medication. The pain is not radiating .
• Then she developed fever 10 days back which was insidious in onset gradually progressive which was high grade and associated with chills and rigors.
• She also had history of vomitings. On day 1 of admission - 1 episode and on day 2 of admission - 6 episodes. They are yellow in colour, food as contents, not projectile. Relieved on medication.
• The patient had noticed red coloured urine before the day of admission and on the day of admission, which is not associated with pain or burning or difficulty in passing urine, no oliguria or increased frequency of micurition .
•She had facial puffiness and abdominal distension on day 5 of admission which later subsided.
• There is no history of chest pain, breathlessness, cough, indigestion and heart burn.
Past history:
At the age of 10years she was diagnosed with Rheumatic heart disease and she underwent a surgery (CABG and mitral valve replacement)following which she took medication for 2 years and she stopped using them thereafter ,and again she’s using the medication from past 7months.
No DM,TB,HTN,Epilepsy
Personal history :
Diet:mixed
Appetite:normal
Bowel and bladder movements:regular
Sleep disturbed due to pain
No addictions
No allergies
Family history :not significant
Menstrual history :
Age of menarche:13 years
5/28 cycle ,regular,moderate flow , with clots ,no dysmenorrhea
Marital history : married for 7 years 7months back gave birth to a girl baby.
General examination:
Patient is conscious,coherent and cooperative
Well oriented to time place and person
Moderately built and nourished
Pallor -present
No icterus ,cyanosis,clubbing ,generalised lymphadenopathy,edema
Vitals:
Pulse rate:70/min
RR:34/min
BP:120/70 mmHg
Temp:afebrile.



Fluid intake and output chart:




Systemic examination:
Per-abdomen examination
Inspection:
Shape of abdomen:normal
Movements:all quadrants are moving equally with respiration
C-section scar is present
No engorged veins ,sinuses,swellings
Striae gravidarum present
No visible gastric peristalsis
Palpation :
No local rise of temperature ,no tenderness
No palpable mass
No hepatomegaly ,spleenomegaly
Kidney ballotable
Percussion :resonant note heard
Auscultation : bowel sounds heard.
Clinical images:



CVS :
Inspection:
Midline scar is present
Shape of chest normal
No precordial bulge
JVP not raised
No visible pulsations
Palpation: Apex beat felt at 5th ICS 2.5 cm lateral to mid clavicular line
Auscultation :
S1S2 heard no murmurs
Click sound is heard without stethoscope (replaced mitral valve ).
Investigations:
On Day1:
Hb:9.8 %
TLC:21,900
N:83,L:7,B:2,M:8
Platelet:2.1 lakh
Normocytic normochromic anemia
LFT:
APTT :51seconds
PT:25 sec
INR:1.8
RBS:101 mg/dL
Urea:26
Sr.creatinine :1.4
Na+:141 mEq
K+:3.4
Cl_:106
On day 4
Hb:10.1
Urea :18
USG :
(Done On the day of admission)
Impression:altered echo texture and increased size of right kidney
 2decho:
2decho:
ECG:

X-ray:

Diagnosis:
Acute pyelonephritis
Treatment:
IV fluid -NS,RL :75mL/hr
Inj.piptaz 2.25 gm IV TID
Inj.pan 4mg IV OD
Inj. Zofer 4mg IV SOS
Inj.neomol 1gm IV SOS (if temp >101F)
Tab.PCM 500mg /PO/QID
Tab .niftaz 100mg /PO / BD (stopped)


This is a case of 50 years old patient, who is a farmer by occupation, resident of pochampally has presented to the casualty 7 days back with the chief complaints of
- Abdominal distension since 8 days
- Pain in the abdomen since 8 days
- Pedal edema since 6 days
5AM WAKE UP
Till 8AM- Field work
8AM- Breakfast (Rice)
1PM - lunch
6PM- reaches home
8PM - dinner
9PM - sleep
The Patient was apparently asymptomatic 6 months ago when he developed jaundice and was treated in a private hospital
His last consumption of alcohol was on 29th May 2022 which was when he drank more than usual
Then he developed abdominal distension which was insidious in onset and gradually progressive to the present size
There were no aggravating and relieving factors
It was associated with
1)pain abdomen in the epigastric and right hypochondriac region which is insidious in onset and diffuse to whole of the abdomen and gradually increased in intensity and is of colicky type
Pain is persistent throughout the day. No history of radiation to the back.
2) bilateral pedal edema below knees and is of pitting type, which was insidious in onset and gradually progressive throughout the day and is maximum in the evening and is not relieved by rest
No local rise of temperature and tenderness
Associated symptoms- shortness of breath since 4 days
There is no history of orthopnoea, PND or palpitations
No history of facial puffiness and haematuria
No history of evening rise of temperature, cough, night sweats
No history suggestive of hemetemesis, melena, bleeding per rectum
No raised JVP, basal lung crepitations
No palpable mass per abdomen
Past history
No history of of similar complaints in the past
Not a known case of Hypertension, Diabetes, asthma, epilepsy, TBNo previous surgical history
Personal historyDiet- MixedAppetite- Decreased since 10 daysBowel and bladder movements- RegularSleep- AdequateAddictions-Patient is a chronic smoker since 30 years- 4to5 beedis/dayAlcohol - Consuming whisky since 20 years- 3 to 4 times per week (90 ml each time)No history of drug or food allergies
Family historyNo similar complaints in the family
General examination
Done after obtaining consent, in the presence of attendant with adequate exposure
Patient is conscious, coherent, cooperative and well oriented to time, place and person
Patient is well nourished and moderately built
Pallor - absent
Icterus- present
Cyanosis- absent
Clubbing- absent
Pedal edema- present- bilateral pitting type
Lymphadenopathy- absent
General examination
Done after obtaining consent, in the presence of attendant with adequate exposure
Patient is conscious, coherent, cooperative and well oriented to time, place and person
Patient is well nourished and moderately built
Pallor - absent
Icterus- present
Cyanosis- absent
Clubbing- absent
Pedal edema- present- bilateral pitting type
Lymphadenopathy- absent
VitalsTemperature- AfebrileBlood pressure- 120/80 mm of HgPulse rate- 78 bpmRespiratory rate- 16 cpm
Local examinationAbdominal examination:
InspectionShape of the abdomen- DistendedUmbilicus- evertedMovements of abdominal wall- moves with respirationSkin is smooth, shinyNo visible peristalsis, pulsations, sinuses, engorged veins, hernial sites Palpation
Inspectory findings are confirmedTenderness is present in whole of the abdomenGuarding and rigidity presentFluid thrill positiveNo hepatosplenomegaly
PercussionFluid thrill- felt Liver span- Not detectable
AuscultationBowel sounds are heard
Cardiovascular system examination:S1 and S2 sounds are heardNo murmurs
Respiratory system examination:Bilateral air entry presentNormal vesicular breath sounds are heard
Central nervous system examination:No focal neurological deficits
Investigations



Investigations:
SerologyHIV- NegativeHCV- NegativeHbsAg- Negative
Hemogram
Haemoglobin- 9.8 gm/dl
Total count- 7200 cells/cummNeutrophils- 49%Lymphocyes- 40%Eosinophils- 1%Monocytes- 10%PCV- 27.4 vol%MCH- 33 pgMCHC- 35.8%RDW- 17.6RBC count- 2.97 millions/cumm
Prothrombin timeProthrombin time- 16 secINR- 1.11
Ascitic fluid protein sugarSugar- 95 mg/dlProtein- 0.6 g/dl
Ascitic fluid for LDHLDH- 29.3 IU/L
Blood UreaBlood urea- 12mg/dl
ESRESR- 15mm/1st hour
LFTTotal bilirubin- 2.22 mg/dlDirect bilirubin- 1.13 mg/dlSGOT(AST)- 147 IU/LSGPT(ALT)- 48 IU/LAlkaline phosphate- 204 IU/LTotal proteins- 6.3 gm/dlAlbumin- 3 gm/dl
Serum electrolytesSodium- 133 mEq/LPotassium- 3 mEq/LChloride- 94 mEq/L
Serum creatinineSerum creatinine- 0.8 mg/dl
APTTAPTT test- 32 sec
SAAGSerum albumin- 3 gm/dlAscitic albumin- 0.34 gm/dlSAAG- 2.66


Provisional diagnosis:Acute decompensated liver failure with ascites
Treatment:1. Inj PAN 40 mg IV/OD2. Inj LASIX 40mg IV/BD3. Tab Spiranolactone 50mg/ BD4. Inj Thiamine 1 amp in 100 ml NS IV/ TID5. Syrup lactulose 15 ml/ TID6. Abdominal girth charting 4th hourly7. Fluid restriction <1L/ day8. Salt restriction <2g/ day



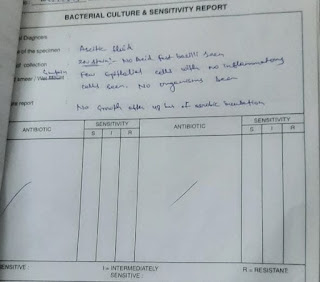
Ascitic fluid tappingAscitic fluid was tapped twice- on 2nd June 2022 & 6th June 2022




{kind=link}
{kind=link}
{kind=link}