LONG CASE
A 55year old female patient who is housewife hailing from nalgonda was brought to the hospital with
CHIEF COMPLIANTS ::
* Fever since 5 days .
* Neck stiffness since 5 days.
HISTORY OF PRESENT ILLNESS ::
Patient was apparently asymptomatic 5 days back and was able to perform her regular activities without any difficulty then she experienced Fever which is
sudden onset
Continuous
Associated with chills and rigor
Associated with generalised body pains and headache .
Associated with 1 episode of vomiting which is non projectile, non bilious , food particles as content and non foul smelling. Not associated with abdominal pain and loose stools.
Relieved on medication.
Neck stiffness which is
Sudden onset
Associated with decreased range of movements at neck
No H/O trauma
Not relieved on rest and painkillers.
No H/O Burning micturition.
PAST HISTORY ::
No similar compliants in the past.
Not a known case of hypertension
Tuberculosis,
epilepsy
asthma
and CAD.
There is H/O CVA with compliants of bilateral upper & lower limb paralysis 7 years back for which she was treated and recovered in 1month .
Surgical H/O - Hysterectomy 25years back.
PERSONAL HISTORY
Diet - Mixed
Appetite - reduced
Sleep - adequate
bladder - regular
Bowel movements - constipation since 3 days
No addictions and no known allergies.
FAMILY HISTORY
Not significant.
GENERAL EXAMINATION
Patient is conscious, coherent, and cooperative.
Moderately built and nourished.
Well oriented to time, place and person.
Patient was examined in supine position in a well lighted room after taking consent and explaining the procedure.
PALLOR - absent
ICTERUS - absent
CLUBBING - absent
CYANOSIS - absent
LYMPHADENOPATHY - absent
EDEMA - absent
VITALS ::
Temperature - 99⁰F
Pulse rate - 98 beats per minute , normal volume , character and normal vessel wall , no radioradial and radiofemoral
delay .
Respiratory rate - 20cycles per minute
Blood pressure - 110/70 mmHg in both arms.
O2 sat. - 96% at room air.
CNS :
Dominance - Right handed
Higher mental functions
• conscious
• oriented to person and place
• memory - able to recognize their family members
• Speech - Normal.
Cranial nerve examination
• 1 - sense of smell present.
• 2- Direct and indirect light reflex present
• 3,4,6 - no ptosis Or nystagmus
• 5- corneal reflex present on both sides
• 7- no deviation of mouth, no loss of nasolabial folds, forehead wrinkling present
No dysphagia and hoarsness
• 8- able to hear
• 9,10- position of uvula visualized
• 11- sternocleidomastoid contraction present
• 12- no tongue deviation
Motor system
Attitude - Normal
Tone - Normal tone on right side(UL,LL)
Normal tone on left side(UL,LL)
Bulk - Rt. Lt.
Arm 26cm. 26cm
Forearm 19cm 19cm
Thigh 42 cm. 42cm
Leg 28cm. 28cm
Power
Right. Left
UL 5/5 5/5
LL. 5/5 5/5
Reflexes Right Left
Biceps + + ++
Triceps + + ++
Knee jerk ++ ++
Ankle jerk ++ ++
Babinski Flexion Flexion
Corneal reflex present on both sides
Light reflex present on both sides
(Direct and indirect)
Sensory system: Normal
Cerebellar signs :
Knee - heel incoordination - No
Finger - nose incoordination- No
Meningeal signs -
Neck stiffness present .
Kernig's sign - positive
Brudzinki sign - positive
Biceps
Triceps
Knee
Power.
Ankle
Babinski
EXAMINATION OF OTHER SYSTEMS
RESPIRATORY SYSTEM:
Chest symmetrical, No paradoxical movements, Normal vesicular breath sounds heard,
No abnormal/added sound
CARDIOVASCULAR SYSTEM:
S1 S2 Heart sounds – normal
No thrills/murmurs
ABDOMINAL EXAMINATION
Abdomen is non tender,soft, ,No organomegaly, No ascites.
Provisional diagnosis:-
Dengue fever with viral meningoencephalitis.
Denovo diabetes mellitus type 2.
MRI brain :
X ray Lateral view of skull and neck-2Decho:-
Treatment:-
Inj. CEFTRIAXONE 2 gm/ BD
Inj.DEXA 6mg/iv/tid
Inj . Vancomycin 1gm/iv
Inj. Pcm 1gm/iv
Tab . Pcm 650 mg
Tab. Ecospirin 75 mg /po/od
Tab. Atorvas 10 mg /po/od
Syp. Cremaffin plus 30ml/po
On day 2 :-
Patient is conscious, coherent, cooperative.
Vitals:-
Temperature: 99°F
Pulse rate: 76bpm
Resp rate:15cpm
BP:130/90mmhg
Spo2:96%
GRBS- 197mg/dl
Treatment-
Inj. CEFTRIAXONE 2 gm/ BD
Inj.DEXA 6mg/iv/tid
Inj . Vancomycin 1gm/iv
Inj. Pcm 1gm/iv
Tab . Pcm 650 mg
Tab. Ecospirin 75 mg /po/od
Tab. Atorvas 10 mg /po/od
Syp. Cremaffin plus 30ml/po
Oint.Diclofenac for thigh pain
On day 3:-
Patient is conscious, coherent, cooperative.
Vitals:-
Temperature: 99°F
Pulse rate: 78bpm
Resp rate:16cpm
BP:120/90mmhg
Spo2:96%
GRBS- 190mg/dl
Investigations:-
Treatment-
Inj. CEFTRIAXONE 2 gm/ BD
Inj.DEXA 6mg/iv/tid
Inj . Vancomycin 1gm/iv
Inj. Pcm 1gm/iv
Tab . Pcm 650 mg
Tab. Ecospirin 75 mg /po/od
Tab. Atorvas 10 mg /po/od
Syp. Cremaffin plus 30ml/po
Oint.Diclofenac for thigh pain
Inj.pan 40 mg iv /od
Tab. Naproxen 250 mg po/tid.
Flexbenz gel for L/A on thighs

--------------------------------------------------------
SHORT CASE
A 51 year old male patient who is a resident of chitayala ,who works is a labourer in a goods company came to the hospital with chief complaints of:Fever since 10 days
Shortness of breath since 10days
Cough since 7 days
HISTORY OF PRESENT ILLNESS :
The patient was apparently a symptomatic 10days back then he developed high grade fever which was insidious in onset associated with chills and rigours and was relieved on taking medications .
The patient was able to walk a kilometer 10 days back and later slowly was facing shortness of breath even after walking for short distances and which became so severe that even at rest he was feeling shortness of breath .Not associated with wheeze ,no Orthopnea,no paraxsomal nocturnal dyspnea ,no pedal Edema.
Cough since 7 days which is productive mucoid in consistency, whitish,scanty in amount ,non foul smelling, non blood stained .more during night time and on supine position.right sided chest pain diffuse ,
intermittent ,dragging, aggravated on cough ,non radiating ,not associated with sweating ,palpitations .
THERE is weight loss which is present ,no loss of appetite
no history of pain abdomen abdominal distension ,vomiting ,loose stools .
no history of burning maturation .
PAST HISOTRY:
patient gives the history of jaundice 20 days back which resolved in a week without any medications .
no history of diabetes, hypertension,tuberculosis,bronchial asthma ,Copd,coronary heart disease ,thyroid disease ,cerebrovascular accident .
FAMILY HISTORY:
no similar complaints in the family
PERSONAL HISTORY:
patient is a chronic smoker smokes a pack of cigarettes since past 25 years .
He is a chronic alcoholic consumes 325ml (quarter ml of whiskey)daily.
no bowel and bladder disturbances .
SUMMARY:
51 year old with fever cough and shortness of breath possible diagnosis
1-pleural effusion
2-pneumonia
GENERAL EXAMINATION :
patient is moderately built and nourished .
he is conscious ,comfortable .no signs of pallor ,cyanosis, icterus ,koilonychia ,lymphadenopathy ,edema .
vitals:
patient is afebrile
pulse -83 beats per minute ,normal volume ,regular rhythm,normal character ,no radio femoral delay.
BP-110/70mmhg,measured in supine position in both arms .
Respiratory rate -22 breaths per min
SYSTEMIC EXAMINATION :
Patient examined in sitting position
Inspection:-
oral cavity- Nicotine staining seen on teeth and gums ,nose,chest movements NORMAL
Respiratory movements appear to be decreased on right Side
Trachea is shifting towards left & Nipples are in 4th Intercoastal space
Apex impulse visible in 5th intercostal space.
NO SIGNS OF VOLUME LOSS
no dilated veins ,scars ,sinuses ,visible pulsations ,
no rib crowding ,no accessory muscle usage .
Palpation:-
All inspiratory findings are confirmed
Trachea is shifted
Apical impulse in left 5th ICS,
1cm medial to mid clavicular line
Respiratory movements decreased on right side
Tactile and vocal fremitus reduced on right side in infra axillary and infra scapular region
Gastrointestinal system :
Inspection -
-Abdomen DISTENDED
-All quadrants of abdomen are equally moving with respiration except Right upper quadrant
No visibe sinuses ,scars , visible pulsations or visible peristalsis
Palpation:
All inspectory findings are confirmed.
No tenderness .
Liver - is palpable 4 cm below the costal margin and moving with respiration.
Spleen : not palpable.
Kidneys - bimanually palpable.
Percussion - normal
Auscultation- bowel sounds heard .
No bruits .
Cardiovascular system -
S1 and S 2 heard in all areas ,no murmurs
Final Diagnosis :
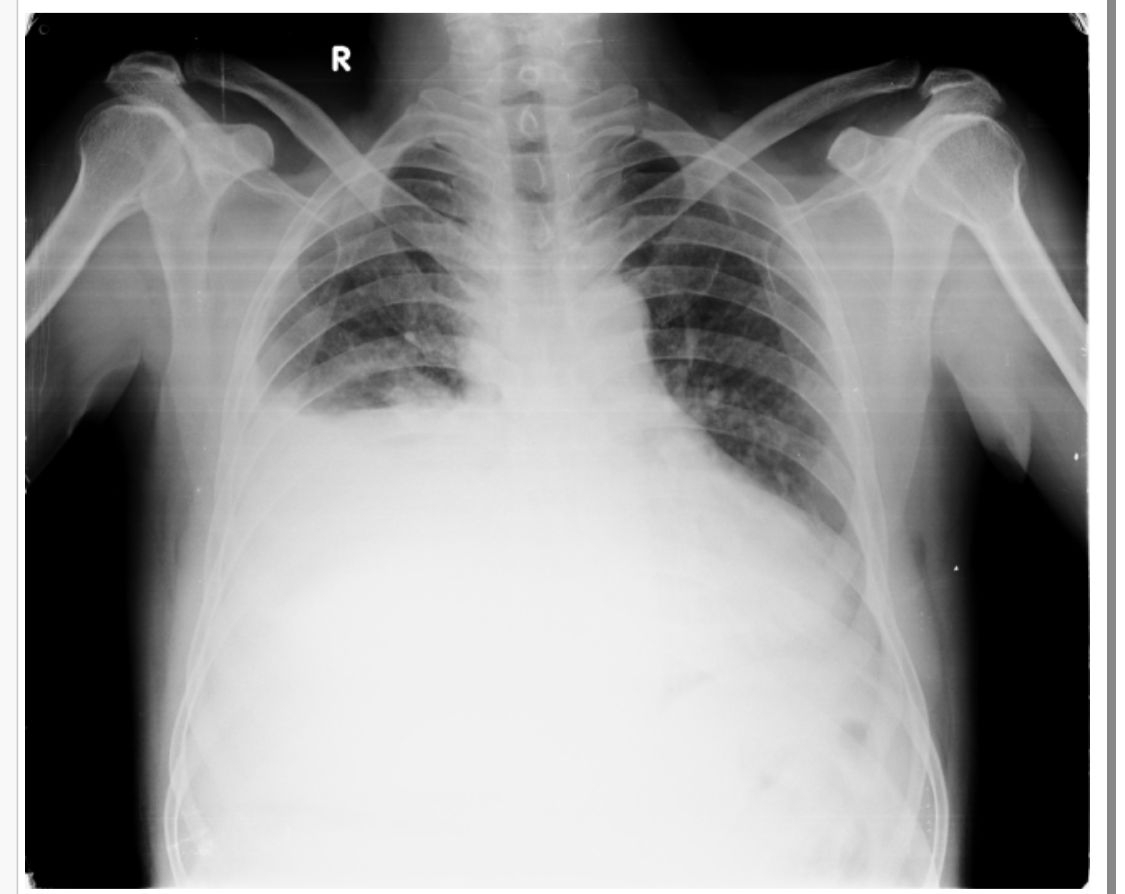
Right sided Pleural effusion likely infectious etiology.
INVESTIGATIONS :
XRAY:CURVED SHADOW AT THE LUNG BASE ,BLUNTIJG THE COSTOPHRENIC ANGLE AND ASCENDING TOWARDS THE AXILLA
SHIFTING DULLNESS IS SEEN ON EXAMINATION
Pleural fluid analysis :
Colour - straw coloured
Total count -2250 cells
Differential count -60% Lymphocyte ,40% Neutrophils
No malignant cells.
Pleural fluid sugar = 128 mg/dl
Pleural fluid protein / serum protein= 5.1/7 = 0.7
Pleural fluid LDH / serum LDH = 0.6
Interpretation: Exudative pleural effusion.
Serology negative
Serum creatinine-0.8 mg/dl
CUE - normal
Final diagnosis :
1.right sided pleural effusion
2. Right lobe liver abscess
Treatment :

































{kind=link}
Comments
Post a Comment