1701006118 CASE PRESENTATION
LONG CASE

The patient was apparently asymptomatic 6 months ago when he developed fever with jaundice and was treated at a private practitioner.
Later he developed Abdominal distension about 7 days ago after consuming unusual amounts of alcohol at a gathering,
- insidious in onset, gradually progressive to the present size - associated with
- Pain in epigastric and right hypocondrium - colicky type.
- Fever - high grade, not associated with chills and rigor, decreased on medication, No night sweats.
- Not associated with Nausea, vomiting, loose stools
There was Pedal edema,
- Pitting type
- Bilateral
- Started at the ankle gradually progressed to below knees
- Increases untill the end of the day - maximum at evening.
- No local rise of temperature and tenderness
- Grade 2
- Not relieved on rest
He also complained of Shortness of breathe since 4 days - MRC grade 4
- Insidious in onset
- Gradually progressive
- Agrevated on eating and lying down ; No relieving factors
- No PND
- No cough/sputum/hemoptysis
- No chest pain
- No wheezing

Patient is a known alcoholic since 20 years. Distention increased after his last drink five days back.
Daily Routine :
Wakes up at 5am and goes to field.
Comes home at 8am and has rice for breakfast. Returns to work at 9am.
1pm - lunch
2-6 pm - work
6pm - home
8pm - dinner
Alcohol- 2 times a week, 180 ml.
PAST HISTORY:
No history of similar complaints in the past
Medical history- not a known case of DM, HTN, TB, Epilepsy, Asthma, CAD
Surgical history - not significant
PERSONAL HISTORY:
- Diet - mixed
- Appetite- reduced since 7 days
- Sleep - disturbed
- Bowel - regular
- Bladder - oliguria since 2 days, no burning micturition, feeling of incomplete voiding.
- Allergies- none
- Addictions -
- Beedi - 8-10/day since 20 years, smoking index= 10×20= 200 ;
Alcohol - Toddy - 1 bottle, 2 times a week, since 20 years;
- Whiskey-180 ml, 2 times a week, since 5 years.
- Last alcohol intake - 29th May, 2022.
FAMILY HISTORY:
Not significant
GENERAL EXAMINATION:
Patient is conscious, coherent and co-operative.
Examined in a well lit room.
Moderately built and moderately nourished
Icterus - present (sclera)

Pedal edema - present - bilateral pitting type, grade 2 - https://youtube.com/shorts/Uwz_0gxzqUM?feature=share
No pallor, cyanosis, clubbing, lymphoedenopathy.




Vitals :
Temperature- febrile
Respiratory rate - 16cpm
Pulse rate - 101 bpm
BP - 120/80 mm Hg.
SYSTEMIC EXAMINATION:
CVS: S1 S2 heard, no murmurs
Respiratory system : normal vesicular breath sounds heard.
ABDOMINAL EXAMINATION:
INSPECTION :
Shape of abdomen- distended
- Umblicus - everted
- Movements of abdominal wall - moves with respiration
- Skin is smooth and shiny;
- No scars, sinuses, distended veins, striae.
PALPATION :
Local rise of temperature present.
Tenderness present - epigastrium.
Tense abdomen
Guarding present
Rigidity absent
Fluid thrill positive
https://youtube.com/shorts/dRnY4B6YVV8?feature=share
Liver not palpable
Spleen not palpable
Kidneys not palpable
Lymph nodes not palpable
PERCUSSION:
Liver span : not detectable
Fluid thrill: felt
AUSCULTATION:
Bowel sounds: heard


CNS EXAMINATION:
Conscious
Speech normal
No signs of meningeal irritation
Cranial nerves: normal
Sensory system: normal
Motor system: normal
Reflexes: Right. Left.
Biceps. ++. ++
Triceps. ++. ++
Supinator ++. ++
Knee. ++. ++
Ankle ++. ++
Gait: normal
INVESTIGATIONS:
SEROLOGY:
HIV - negative
HCV - negative
HBsAg - negative
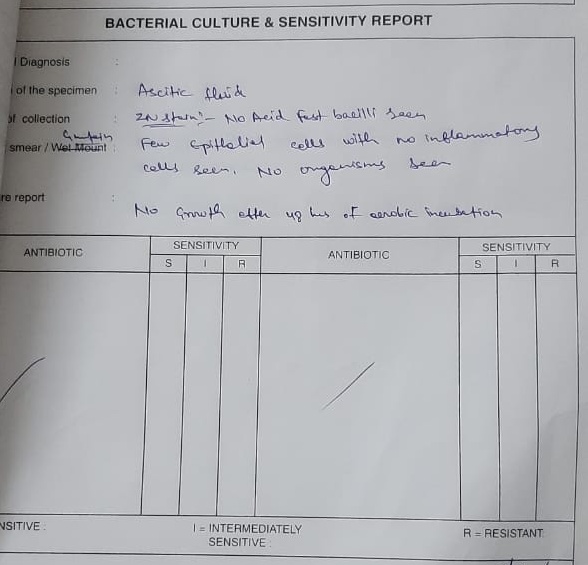
ASCITIC TAP:
ASCITIC FLUID CYTOLOGY:

CULTURE AND SENSITIVITY:
ECG:

HEMOGRAM:













PROVISIONAL DIAGNOSIS:
Decompensated chronic liver failure with ascites secondary to alcohol consumption.
TREATMENT:
Inj. Pantoprazole 40 mg IV OD
Inj. Lasix 40 my IV BDI
Inj. Thiamine 1 Amp in 100 ml IV TID
Tab. Spironolactone 50 mg BB
Syrup Potchlor 10ml PO TID
Syp. Lactose 15ml TID
Abdominal girth charting - 4th hourly
Fluid restrictriction less than 1L per day
Salt restriction less than 2 gms per day



A 56 year old male patient, daily wage worker by occupation, resident of Nalgonda came to opd with
CHIEF COMPLAINTS :
1. Pain abdomen since 20 days.
2. Multiple abdominal swellings since 7 days.
3. Fever since 7 days
HISTORY OF PRESENT ILLNESS :
Patient was apparently asymptomatic 5 months back, then he developed Dry cough which was insidious in onset, gradually progressive and there was no sputum. Later, he developed fever which was high grade, associated with chills and rigors. He went to the hospital with above complaints and medications were prescribed and the symptoms subsided.
After 2 months, patient observed loss of weight and loss of appetite for which he went to the doctor. Upon, his advice, the patient got tested for Tuberculosis and HIV. He tested positive for both TB and HIV. The patient was given ART and ATT.

20 days back, patient started experiencing
- Pain around the umbilicus which was insidious in onset gradually progressive associated with abdominal discomfort.
- Patient also complains of small multiple swellings in the abdomen since 7 days which hav gradually increased to present size.
- He had fever since 7 days, high grade associated with chills and rigors.

PAST HISTORY :
Patient is a known case of Tuberculosis and HIV-AIDS and is on regular treatment.
Patient is not a known case of Diabetes mellitus, Hypertension, Asthma, Epilepsy, Thyroid disorders.
There is no surgical history, no history of blood transfusions.
TREATMENT HISTORY:



PERSONAL HISTORY :
Diet : Mixed
Appetite : Decreased
Sleep : Adequate
Bowel and Bladder movements : Regular
Addictions : None
FAMILY HISTORY :
No history of similar complaints in the family.
HISTORY OF ALLERGIES :
No known drug or food allergies.
GENERAL PHYSICAL EXAMINATION :
Patient is conscious, coherent, co-operative and well oriented to time, place and person.
Moderately built and moderately nourished.




LYMPH NODE EXAMINATION:
Lymphadenopathy is present. There are multiple enlarged lymph nodes in abdomen and neck.
Cervical lymph nodes:
Right side--
Level 5 nodes are positive - lymph nodes in the posterior triangle of neck
3×2cm, mobile, soft to firm in consistency, non matted
Left side--
Level 4 lymph nodes- lower jugular lymph nodes are positive
2×1cm, mobile, soft in consistency, non matted

Inguinal lymph nodes:
Right side--
Right inguinal lymph nodes positive
2-3 in number, 1×1 cm, soft, non tender
Left side--
Left inguinal lymph nodes positive,
3-4 in number, 1×1cm, soft, non tender

Axillary nodes are not palpable.
Vitals :
Temperature : Afebrile
Pulse Rate : 86 bpm
Blood Pressure : 120/80 mm Hg
Respiratory rate : 16 cpm
GRBS : 106 mg/dl

SYSTEMIC EXAMINATION :
Cardiovascular System : S1, S2 heard. No murmurs.
Respiratory System : Normal Vesicular Breath Sounds heard.
Central Nervous System : Conscious, Alert, Speech normal, Motor and Sensory examination normal.
Per Abdomen : Soft. No hepatomegaly. No splenomegaly.
INVESTIGATIONS :








ECG report:

Chest x-ray

2D Echo

FNAC : From right cervical lymph node - acid fast bacilli positive
PROVISIONAL DIAGNOSIS :
Fever with generalized lymphadenopathy secondary to HIV/TB
TREATMENT :
1. Tab. Dolo 650 PO TID
2. Tab. MVT OD
3. Inj. Neomol 1g IV/SOS
4. Tab. Dolutegravir, Lamivudine, Tenofovir Disoproxil Funerate (50 mg,300 mg,300 mg) PO OD
5. Tab. Rifampicin, Isoniazid, Pyrazinamide, Ethambutol (150 mg,75 mg,400 mg,275 mg) PO OD
6. Tab. Septran-DS PO BD
7. Tab. Pan 40 mg PO BD
8. Syrup Aristozyme PO 10 ml TID



{kind=link}