1701006120 CASE PRESENTATION
LONG CASE
A 46yr old male was resident of nalgonda , farmer by occupation was brought to medicine OPD with complaints of :
Chief compliants:
Burning micturition present since 10 days
Hiccups since 3 days
Vomiting since 2 days
Giddiness, drowsiness and deviation of mouth to right since yesterday night
HOPI:
Pt was apparently asymptomatic
10yrs back pt had c/o polyuria and was diagnosed with Type 2 DM, started on Oral hypoglycemic agents 10 yr back, which pateint has been taking on and off due to financial crises.
Oral hypoglycemic agents were converted to insuline and pt underwent cataract surgery 3 yrs ago . Pt has been taking insulin three times a day befor food regularly.
h/o small injury on leg which gradually progressed to non healing ulcer extending upto below knee which turned into wet gangrene , eventually ended with below knee amputation 1yr back.
Delayed Wound healing present- wound healing took 2 months time to heal.
10 days back ,then he developed burning micturation , not associated with fever and decreased urine output.
3 days back then pateint complaints of hiccups
2 days back, then pt developed c/o vomiting ,had 4-5 episodes, containing food particles,non bilious.
Pt c/o deviation of mouth and giddiness since yesterday night(18/05/2022) and was brought to the hospital and GRBS was checked which was high, for which he was given NPH 10 IU and HAI 10 IU
No c/o fever/cough/cold/ abdominal pain
No c/o chest pains/palpitations/syncopal attacks

Past history:
Not a k/c/o HTN/Epilepsy/TB/BA/Thyroid disorder/CAD/CVD
Not on any other medication
No h/o blood transfusion
Personal History:
Married
Appetite-Normal
Diet-Vegetarian
Sleep - adequate
Micturition- burning micturition present.
Bowel- regular.
DIET OF THE PATIENT:
Patient take three meals.
Morning has idly , dosa , vada any sort of tiffin.
Afternoon has rice curd vegetable dal.
Night has jawal.
No smalls meals...patient takes biscuits whenever he experiences an hypoglycemic attack ( feeling of giddiness , sweating )
Habits/Addiction:
Alcohol-
Not consuming alcohol since 1 yr.
Previously (1yr back) Regular consumption of alcohol, about 90mL whiskey consumed almost daily.
Family history:
Not significant
General Examination:
Pt examined in well lit room and with informed consent
Pt is conscious, cooperative and coherent and we'll Oriented to time place person.
Well built and moderately nourished
Pallor present
No icterus/Cyanosis/Clubbing/Koilonychia/Lymphadenopathy/Edema
No signs of dehydration



Vitals at the time of Admission:
BP: 110/80 mmHg
HR: 98 bpm
RR: 18 cpm
TEMP: 101F
SpO2: 98% on RA
GRBS: 124 mg/dL
Systemic Examination:
ABDOMEN EXAMINATION
INSPECTION:
Shape – scaphoid
Flanks – full
Umbilicus –central , inverted.
All quadrants of abdomen are moving with respiration.
No dilated engorged veins
No visible pulsations, visible peristalsis and scars.
PALPATION:
No local rise of temperature and tenderness
All inspectory findings are confirmed.
No guarding, rigidity
Deep palpation-
Liver : palpable just below costal margin ( right)
Sleep : not palpable
Kidney : not palpable
PERCUSSION:
There is no free fluid
Percussion of liver for liver span : 12cm
Percussion of spleen- dull note
AUSCULTATION:
Bowel sounds heard.
Other systems:
CVS: S1S2 heard, No murmurs
RS: BAE+,NVBS
CNS:
Higher function test:
Slurred speech
Cranial nerves : intact
Motor system :
1, Bulk : right. Left
Upperlimb normal. Normal
Lowerlimb. thigh -N. Normal
Below knee amputated on R side
2, Tone :
Upperlimb. Normal. Normal
Lowerlimb. Normal. Normal
3, Power :
Neck:. Normal
Trunk:. Normal
Upper limb 5 5
Lower limb 5 5
4, Reflexes
Right Left
Biceps 2+. 2+
Triceps 2+ 2+
Supinator. 2+ 2+
Knee 2+. 2+
Ankle 2+. 2+
Planter reflex Amputated flexion
Sensory system : normal
Meaningal signs : negative


Investigations:
19/05/2022: ( on admission)
X ray KUB:
.png)
CT scan
.png)
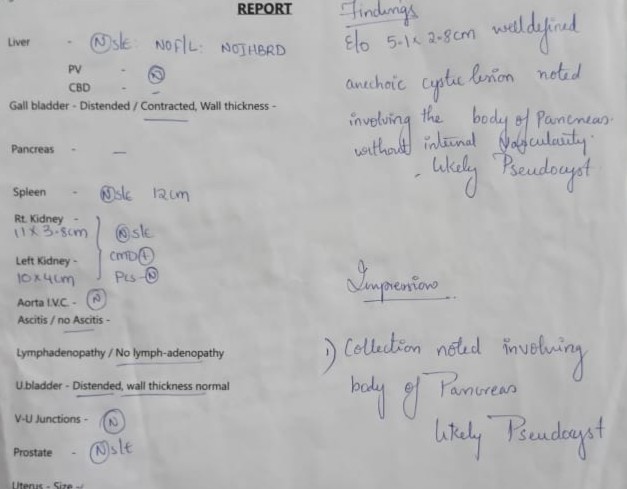
USG abdomen pelvis

Urine examination:


Complete blood picture:

Liver function test:

.png)


.png)








A 22yr old male pt. painter by occupation resident of nalgonda came with
Cheif complaints:
Pain abdomen since 4 days.
HOPI:

Pt. Has started consuming alcohol 4 yrs back due to peer pressure , intially taking one peg per day which has increased to 90ml morning and evening i. e twice daily. He has stopped consuming alcohol 3 months back as advised by the doctor.
Pt. Has history of smoking since 2 yrs . He has been smoking beedies 5 per day till date.
Pt was apparently asymptomatic 3 months back then he developed abdominal pain which was dragging in character for which he was admitted in near by hospital in nalgonda . He was diagnosed with acute pancreatitis and was treated inadequately and was advised to stop consumption of alcohol.
Since then pt has stopped consuming alcohol and has been experiencing alcohol withdrawal symptoms like getting angry , agitation , irritability , craving to consume alcohol, tremors . Pt had consumed alochol 4 days back due to fight with his wife.
In veiw of this symptoms pt.has been brought to psychiatry OPD for deaddiction. He was referred to medicine OPD in veiw of pain abdomen.
Pain was , insidious in onset , started after consuming of alcohol in epigastrium and left hypochondrium which was relieved on bending forward and lying down , aggregated on eating food and standing straight.
No h/o fever , nausea , vomiting.
No h/o chestpain , shortness of breath , constipation
Flatus passed
Past history:
H/o similar complaint in past 3 months back.
No other co morbid conditions
No h/o previous medical surgical history.
Family history :
Not significant
Personal history
Diet : mixed
Appetite : normal
Bowel bladder: regular
Sleep: inadequate
General examination:
Pt was concious coherent and cooperative
Thin built and moderately nourished
Pallor - present
No icterus,cyanosis , clubbing,lymphadenopathy, edema





Nasogastric tube has been placed which is attached to the bag
Vitals at the Time of admission
Temperature- afebrile
Pulse rate- 94bpm
Blood pressure-120/80mmHg
Respiratory rate- 16cpm
Systemic examination:
Abdominal examination:
Inspection:
Shape of the abdomen- flat
Umbilicus is central
No visible scars,pulsations, peristalsis, engorged veins
Palpation:
All the inspectory findings are confirmed.
Tenderness present over the epigastrium and left hypochondrium region
Liver palpable 2cms below costal margin
Liver span: 11.5cm ( normal)
Spleen : not palpable
Kidney : not palpable
Percussion:
No free fluid
Ascultation:
Bowel sounds heard
Other systems:
Respiratory:
b/l air entry present , no added breath sound
CVS :
S1 S2 heard , no added murmurs
CNS :
Higher function intact
No motory and sensory deficit.
Cranial nerves normal .
Investigations:
USG abdomen
Serum amylase : increased to more than three times
Serum lipase


Other tests :
Hemogram
RBS
RFT
LFT
Blood grouping




Diagnosis:
Pseudocyst of pancreas secondary to unresolved acute pancreatitis.
Treatment:
Nil per oral
IV fluids Ringer lactate ,Normal saline 100 ml per hour
Inj. Tramadol100mg in 100ml NS IV BD
Inj.pantop 40 mg IV OD
Inj. Optineurin 1 ampoule in 100ml NS IV OD
Psychiatry medication
Tab . Lorazepam 2mg BD
Tab . Benzothiamine100mg OD







Comments
Post a Comment