1701006151 CASE PRESENTATION
LONG CASE :
A 35 year old male, bartender by occupation, resident of Sathupalli, Khammam district, came to the hospital with the following chief complaints --
- shortness of breath - from 10 days
- cough- from 2 days
- palpitations - from 7 days
- 1 month ago, he developed shortness of breath while lying down, then he visited local RMP, where he was given an injection? and symptoms subside for a while. He experienced symptoms after consumption of alcohol.
- insidious onset
- mucopurulent
- sudden in onset
- no associated with chest pain
- NO history of similar complaints in the past.
- Not a known case of Diabetes, Hypertension, Tuberculosis, Asthma, hypothyroidism/hyperthyroidism, COPD, and blood transfusions.
- no history of previous surgeries'
- Diet: mixed
- Appetite: reduced from past 10 days
- Bowel habits: normal
- Bladder habits: normal
- Sleep: disturbed from past 10 day
- Addictions:
- Built and nourishment: moderately built and moderately nourished
- Pallor: No pallor
- Icterus: No icterus
- Cyanosis: No cyanosis
- Clubbing: No clubbing
- Generalized lymphadenopathy: No generalized lymphadenopathy
- Pedal edema: No pedal edema
- Temperature afebrile
- Pulse 140-160 bpm (irregularly irregular)
- Respiratory rate : 30 per minute
- Bp 130/90
- Spo2 98%
- GRBS 132 mg%
- The chest wall is bilaterally symmetrical
- No dilated veins, scars.
- Apex beat is shifted to 6th inter coastal space , 2-3cm deviated from mid clavicular line
- parasternal heave not felt
- thrill not felt
- Right and left borders of the heart are percussed
- S1 and S2 heart sounds heard
- RESPIRATORY SYSTEM EXAMINATION :
- Inspection:
- Shape- elliptical
- B/L symmetrical ,
- Both sides moving equally with respiration .
Palpation:- Trachea - central
- Expansion of chest is symmetrical.
- Vocal fremitus - normal
Percussion:- resonant bilaterally
Auscultation:- bilateral air entry present.
- wheeze is present in all areas
3. ABDOMINAL EXAMINATION:Inspection:- Shape – elliptical
- Umbilicus –everted
- All quadrants of abdomen are moving with respiration.
- No dilated veins, hernial orifices, sinuses
- No visible pulsations.
- Chest is moving normally with respiration.
Palpation :
- No local rise of temperature and tenderness
- All inspectory findings are confirmed.
- No guarding, rigidity
Percussion:
- There is no fluid thrill , shifting dullness.
- Percussion of liver for liver span
- Percussion of spleen- dull note
Auscultation:
- Bowel sounds are feeble.
4.CENTRAL NERVOUS SYSTEM EXAMINATION:
HIGHER MENTAL FUNCTIONS:
Patient is Conscious, well oriented to time, place and person.
Superficial reflexes and deep reflexes are present , normal
Gait is normal
No involuntary movements
Sensory system - all sensations ( pain, touch, temperature, position, vibration sense) are well appreciated .
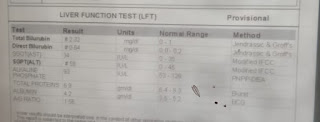
Investigations:





 X RAY :
X RAY :



 Provisional diagnosis:This is a case of atrial fibrillation and dilated cardiomyopathy.TREATMENT :
Provisional diagnosis:This is a case of atrial fibrillation and dilated cardiomyopathy.TREATMENT :- inj AMIODARONE 900mg in 32 ml normal saline @ 0.5mg\min
- inj AUGMENTIN 1.2gm\IV\BD
- tab AZITHROMYCIN 500mg PO\BD
- inj HYDRODRT 100mg IV\BD
- neb with DUOLIN @ 8th hourly
BUDSCORT @ 8th hourly- inj LASIX 40mg\IV\BD
- inj THIAMINE 200mg in 50ml normal saline IV\TID
- tab CARDARONE 150mg
------------------------------------------------- - SHORT CASE
22 Year old Male patient came to the opd with the chief complaints of abdominal pain since 4 days.
History of presenting Illness:
Patient was apparently asymptomatic 4 months back then he developed pain abdomen and vomiting on presenting to a hospital diagnosed as Acute Pancreatitis. He was treated at the hospital and was discharged with the advice to stop drinking alcohol. Then 4 days back , he developed pain over upper abdomen which is of dragging type, radiating to back aggravated on lying down and after eating meals.
The pain increases in sleeping prone position than sleeping than sleeping in supine postion
Patient denies history of fever, nausea, vomiting and diarrhoea.
Patient also gives history of alcohol withdrawal symptoms after the pancreatits episode 4 months back and desries to take up a treatment for deaddiction
Past History:
Not a known case of Diabetes mellitus, Hypertension. Epilepsy,
Cardiovascular diseases. Asthma and tuberculosis
Family History:
No similar complaints in family
Not significant
Personal history:
Takes mixed diet, has early satiety
Sleep is Adequate
Bowel and bladder habits are regular
Addictions: Started drinking alcohol 4 years back with friends started taking alcohol daily since 3 years.
Reduced intake since 3 months. Last intake
was 5 days back of about 250 ml of alcohol.
Smokes 5 beedies per day
General physical examination:
Patient is conscious, cooperative and well oriented to time, place and person.He is thin built.
There is no pallor.
No signs of icterus, cyanosis, clubbing. lymphadenopathy
edema - present
Vitals:
Patient is afebrile
Pulse rate: 92 bpm
Blood pressure: 110/80 mm of Hg
Respirtaory rate: 14 cpm
Systemic Examination:
ABDOMEN EXAMINATION
INSPECTION:
Shape – Flat
Umbilicus –central in position
All quadrants of abdomen are moving equally with respiration.
No dilated veins, hernial orifices, sinuses
No visible pulsations.
A swelling on the left medial coastal border is seen on inspection.

Swelling does not move on respiration.

PALPATION:
Lower margin of the swelling is well defined than upper margin.
No local rise of temperature and tenderness
No guarding, rigidity
Deep palpation- no organomegaly.
PERCUSSION:
There is no fluid thrill , shifting dullness.
Percussion over abdomen- tympanic note heard.
AUSCULTATION:
Bowel sounds are heard.
Respiratory system: Bilateral air entry present,No added breath soundsCardiovascular system: S1, S2 heard, no murmursCentral nervous system: Higher function intactSensory and motor system intactCranial nerves normalInvestigations:
Serum Lipase: 112 IU/L (13-60)
Serum Amylase: 255IU/L (25-140)
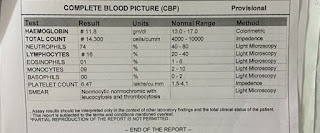
Hemogram:
Hemoglobin: 11.8 mg/dl
Total leucocytes: 14,300 cells/cumm
Lymphocytes: 16(18-20)









Provisional diagnosis: Acute pancreatitis
Treatment:



Nill By Mouth
Intravenous fluids Ringer lactate and normal saline 10ml per hour
Inj. TRAMADOL 100 mg in 100ml normal saline IV BD
INJ. ZOFER 4mg IV BD
INJ. PAN 40 MG IV BD
INJ. OPTINEURIN 1amp in 100 ml nd IV OD
Psychiatric medication:
TAB. LORAZEPAM 2mg BD
TAB. BENZOTHIAMINE 100mg OD


































Comments
Post a Comment