1701006175 CASE PRESENTATION
LONG CASE
A 75 Year old female, farmer by occupation, resident of Nalgonda , came to casualty on 9th June 2022 with chief complaints of-
CHIEF COMPLAINTS:
1. Nausea and vomitings since morning
2. Giddiness since morning
HISTORY OF PRESENTING ILLNESS:

Patient was apparently asymptomatic 6 years ago then she developed symptoms such a Generalized weakness, headache for which she went to hospital and was diagnosed with Diabetes and Hypertension. She was prescribed medicines for it.
Since 4 days she missed her medications as she went to visit her relatives.
On presentation( 9/06/2022),
she complained of 2-3 episodes of vomiting, non-bilious, non-projectile, followed by giddiness.
She was taken to a local hospital primary, where she was found to have GRBS-394 mg/dl and ketone bodies +ve.
No h/o Chest pain, palpitations, syncopial attacks.
No h/o Shortness of Breath.
No h/o Pain abdomen, burning micturition or loose stools.
DAILY ROUTINE

PAST HISTORY
No history of similar complaints in the past.
Patient is a known case of HTN and DM and is on prescribed medications.
H/o Cataract surgery in right eye 3 years ago and in left eye 2 years ago.
Not a known case of CAD, Bronchial asthma, Epilepsy, TB.
No h/o any previous surgeries.
PERSONAL HISTORY
DIET - Mixed
APPETITE- Normal
SLEEP - Adequate
BOWEL AND BLADDER- Regular
ADDICTIONS - No addictions
No known allergies
FAMILY HISTORY
Insignificant
GENERAL EXAMINATION
Patient was examined in a well lit room after taking informed consent.
She is conscious, coherent and cooperative; moderately built and well nourished.
No icterus, clubbing, cyanosis, lymphadenopathy, edema.





VITALS on 9/06/2022
- BLOOD PRESSURE: 230/100 mmHg
- PULSE PRESSURE: 90 Bpm
- RESPIRATORY RATE: 18cpm
- TEMPERATURE: Aferbile
- SpO2: 97% on Room air
- GRBS: 393mg/dl
SYSTEMIC EXAMINATION
1. RESPIRATORY SYSTEM
INSPECTION - No tracheal deviation, Chest bilaterally symmetrical. Thoraco abdominal type of respiration. No dilated veins, pulsations, scars or sinuses.
PALPATION - No tracheal deviation, normal vocal fremitus on both sides.
PERCUSSION - Resonant in all areas.
AUSCULATION - Normal vesicular breath sounds, bilateral air entry present.
2. CARDIOVASCULAR SYSTEM
INSPECTION :- No visible pulsations, no visible apex beat, no visible scars.
PALPATION :- Apex beat felt
AUSCULATION :- Mitral area, tricuspid area, pulmonary area, aortic area - S1, S2 heard.
3. ABDOMINAL EXAMINATION -
INSPECTION - Abdominal distension is present, umbilicus is normal. All quadrants are moving equally with respiration. No visible scars, sinuses, pulsations, engorged veins.
PALPATION - No local rise of temperature or tenderness in all quadrants. No organomegaly.
PERCUSSION - No shifting dullness
AUSCULATION - Bowel sounds and heard, no bruit.
4. CNS -
- Higher mental functions - Normal
- Cranial never functions - Normal
- Sensory system - Sensitive
- Motor system Right Left
LL. 5/5. 5/5
TONE-. UL. Normal. Normal
LL. Normal. Normal
REFLEXES-
Superficial reflexes - Intact
Plantar. Flexion. Flexion
Deep tendon reflexes -
Biceps -. ++. ++
Triceps-. ++. ++
Supinator. ++. ++
Knee. ++. ++
Ankle. ++. ++
GAIT - Normal
- Cerebellar system - Intact
INVESTIGATIONS
1. RANDOM BLOOD SUGAR - 164 mg/dl
2. GLYCATED HEMOGLOBIN (HB1AC)- 6.5%
3. BLOOD UREA - 26 mg/dl
4. SERUM CREATININE- 1.0 mg/dl
5. SERUM ELECTROLYTES-
On 9/06/2022
- Sodium - 139mEq/L
- Potassium - 3.3mEq/L
- Chloride - 98mEq/L
On 11/06/2022
- Sodium - 134mEq/L
- Potassium - 3.6mEq/L
- Chloride - 99mEq/L
On 12/06/2022
- Sodium - 138mEq/L
- Potassium- 3.4mEq/L
- Chloride- 99mEq/L
6. COMPLETE URINE EXAMINATION
On 9/06/2022
- Colour: Pale Yellow
- Appearance: Clear
- Reaction: Acidic
- Specific Gravity : 1.010
- Albumin: ++
- Sugar: ++++
- Bile Salta and Pigments: Nil
- Pus cells: 3-6 /HPF
- Epithelial cells: 2-4 / HPF
- Red blood cell: NIL
- Casts: NIL
7. URINE FOR KETONE BODIES -
On 9/06/2022
Positive
On 11/06/2022
Negative
8. HEMOGRAM
- Hemoglobin: 11.3mg/dl
- Total leucocyte count: 8900cell/cumm
- Neutrophils: 80%
- Lymphocytes:13%
- Eosinophils:02%
- Monocytes:05%
- PCV: 33.7 Volume%
- MCV: 75.4fl
- MCH: 25.3pg
- MCHC: 33.5%
- Platelet Count: 2.67 lakhs/cumm
- RBC Count: 4.47million/cumm
- PBS- Normocytic Normochromic
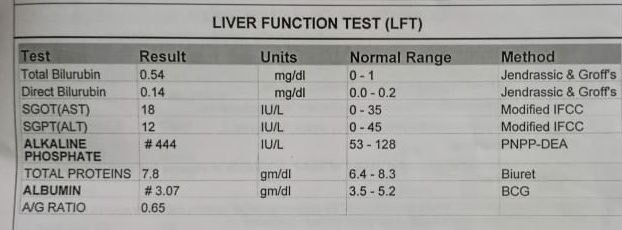
9. LIVER FUNCTION TESTS:
- Total bilirubin: 0.74mg/dl
- Direct bilirubin: 0.18mg/dl
- Aspartate transaminase: 29IU/L
- Alkaline phosphate: 143IU/L
- Alanine transaminase: 11IU/L
- Total proteins: 7.7g/dl
- Albumin: 4.1g/dl
- A/G ratio: 1.16
10. ABG Analysis
- pH : 7.44
- pCO2 : 30.6mmHg
- pO2. :71.4mmHg
- HCO3:22.6mmol/L
- BEB: -2.0mmol/L
- BEecf: -2.8mmol/L
- TCO2: 40.5VOL
- O2 Count: 18.0vol%
- O2sat:93.8%
11. Seronegative for HIV, HEPATITIS B and C
12. USG- Mild hepatomegaly
13. ECG:


PROVISIONAL DIAGNOSIS
Diabetic Ketosis with Hypertensive Urgency
TREATMENT
9/06/2022
- Intravenous fluids normal saline/ ringer lactate @100ml/hr
- Injection Human actrapid insulin I.V infusion @6ml/hr
- Inj. OPTINEURON 1 ampoule in 100ml NS (IV)/ OD
- Inj. ZOFER 4mg IV/ TID
- Tab. NICARDIA 20mg PO/ STAT
- Monitor GRBS, PR, BP, RR CHARTING hourly
- Strict input output charting
10/06/2022
- Intravenous fluids NS 2 @ 100ML/hr
- Injection Human actrapid insulin I.V infusion @6ml/hr
- Inj. OPTINEURON 1 ampoule in 100ml NS (IV)/ OD
- Inj. ZOFER 4mg IV/ TID
- Tab TELMA- AM (40/5) mg PO OD
- MONITORING GRBS,BP,PR, RR CHARTING
- Strict Input output charting
11/06/2022
- Intravenous fluids NS 2 @ 75mL/hr
- Injection Human actrapid insuin 10/10/10 and NPH 8/-/8 ,strict GRBS monitoring
- Inj. OPTINEURON 1 ampoule in NS (IV)/ OD
- Inj. ZOFER 4mg IV/ TID
- Tab CINOD-T (40/10) mg PO OD
- BP 2nd hourly charting
- Strict input/output charting
12/06/2022
- Injection Human actrapid insulin 12/12/12 and NPH 10/-/10, Strict GRBS monitoring
- Inj. OPTINEURON 1 ampoule in NS (IV)/ OD
- Inj. ZOFER 4mg IV/ TID
- Tab CINOD-T (40/10) mg PO OD
- BP 2nd hourly charting
- Strict input/output charting
13/06/2022
- Injection Human actrapid insulin 12/12/12 and NPH 10/-/10, Strict GRBS monitoring
- Inj. OPTINEURON 1 ampoule in NS (IV)/ OD
- Inj. ZOFER 4mg IV/ TID
- Tab CINOD-T (40/10) mg PO OD
- BP 2nd hourly charting
- Strict input/output charting




A 22yr old male patient, painter by occupation , resident of nalgonda came with
CHIEF COMPLAINTS:
Pain abdomen since 4 days.
HISTORY OF PRESENTING ILLNESS:
5 YEARS AGO
Pt. Has started consuming alcohol 4 yrs back due to peer pressure , intially taking one peg per day which has increased to 90ml morning and evening i. e twice daily. He has stopped consuming alcohol 3 months back as advised by the doctor.
2 YEARS AGO
Pt. Has history of smoking since 2 yrs . He has been smoking 5 beedis/per day till date.
3 MONTHS AGO
Pt was apparently asymptomatic 3 months back then he developed abdominal pain which was dragging in character for which he was admitted in near by hospital in nalgonda . He was diagnosed with acute pancreatitis and was treated inadequately and was advised to stop consumption of alcohol.
Since then pt has stopped consuming alcohol and has been experiencing alcohol withdrawal symptoms like getting angry , agitation , irritability , craving to consume alcohol, tremors .
4 DAYS AGO
Pt had consumed alcohol 4 days back due to fight with his wife.
On 7/6/2022
In veiw of this symptoms pt.has been brought to psychiatry OPD for deaddiction. He was referred to medicine OPD in veiw of pain abdomen.
Pain was , insidious in onset , started after consuming of alcohol in epigastrium and left hypochondrium which was relieved on bending forward and lying down , aggregated on eating food and standing straight.
No h/o fever , nausea , vomiting, sweating.
No h/o Chest pain , shortness of breath , constipation
Flatus passed

PAST HISTORY:
H/o similar complaint in past 3 months back.
Not a known case of DM, HTN, BA, Epilepsy, TB.
No h/o previous surgeries
FAMILY HISTORY :
Insignificant
PERSONAL HISTORY
- DIET : mixed
- APPETITE : decreased
- BOWEL AND BLADDER: regular
- SLEEP: inadequate
GENERAL EXAMINATION :
Patient was examined in a well lit room. Henwas conscious, coherent and cooperative; Thin built and moderately nourished
Pallor - present

No icterus, cyanosis , clubbing, lymphadenopathy, edema
VITALS- at the Time of admission
- Temperature- afebrile
- Pulse rate- 94bpm
- Blood pressure-120/80mmHg
- Respiratory rate- 16cpm
SYSTEMIC EXAMINATION

1. ABDOMINAL EXAMINATION
Inspection:
- Shape of the abdomen- flat
- Umbilicus is central
- No visible scars,pulsations, peristalsis, engorged veins
Palpation:
- All the inspectory findings are confirmed.
- No local rise of temperature
- Tenderness present over the epigastrium and left hypochondrium region
- Liver palpable 2cms below costal margin
- Liver span: 11.5cm ( normal)
- Spleen : not palpable
- Kidney : not palpable
Percussion:
- No free fluid
Auscultation:
- Bowel sounds heard
2. RESPIRATORY SYSTEM - Normal vesicular breath sounds heard
3. CVS : S1 S2 heard , no added murmurs
4. CNS : Higher function intact ,No motor and sensory deficit, Cranial nerves normal .
INVESTIGATIONS:
1. USG ABDOMEN:

2. SERUM LIPASE : increased to more than three times - 112 IU/L
3. SERUM AMYLASE-255 IU/L
4. HEMOGRAM:

5. RANDOM BLOOD SUGARS: 97mg/dl
6. RENAL FUNCTION TESTS:

7. LIVER FUNCTION TESTS:
8. BLOOD GROUPING: O+ve
DIAGNOSIS
Pseudocyst of pancreas secondary to unresolved acute pancreatitis.
TREATMENT:
- Nil per oral (NPO)
- IV fluids RINGER LACTATE ,Normal saline 100 ml per hour
- Inj. TRAMADOL 100mg in 100ml NS IV BD
- Inj. PANTOP 40 mg IV OD
- Inj. OPTINEURIN 1 ampoule in 100ml NS IV OD
Psychiatric Medications
- Tab . Lorazepam 2mg BD
- Tab . Benzothiamine100mg OD





Comments
Post a Comment