1801006005 CASE PRESENTATION
long case
A 30-year-old female, a farmer by occupation from Choutuppal, presents to the medicine OPD with complaints of generalized weakness for the past month. stomach pain for the past 4 days and non-projectile vomiting for the past 2 days. The weakness is progressive and has been affecting the patient's ability to perform daily activities. The patient reports that the stomach pain is diffuse, throbbing in type ,intermittent, and associated with nausea aggravated during eating . The vomiting is non-projectile, occurs after meals,non bloodstained and consists of partially digested food.
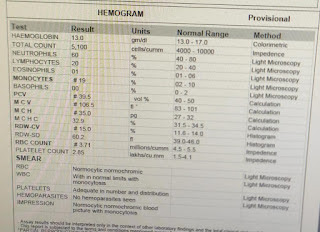
The patient reports that one month ago, she had an episode of fever that was intermittent in nature and accompanied by chills and rigors. She also experienced vomiting 2-3 times a day and small volume watery diarrhea,non blood stained for 10 days. At that time, the patient sought medical attention and was incidentally found to have a hemoglobin level of 5 g/dL. However, the patient was not willing to be admitted to the hospital and was prescribed oral iron medications by the treating physician. H/o dyspnea insidious in onset gradually progressed to grade 3.H/o weight loss pas 1 month No h/o urgency,hesitancy ,burning micturition.No h/o orthopnea,paroxysmal nocturnal dyspnea.No h/o bleeding manifestations
History of Daily Routine: The patient reports waking up at 6:00 AM and drinking tea. After freshening up, the patient cooks and eats breakfast which typically includes rice. The patient walks to work at 8:00 AM and spends the day planting trees and picking cotton from the plants. The patient eats lunch at 12:00 PM, which is typically a curry with rice. The patient returns home at 4:00 PM and performs household chores. The patient eats dinner and goes to sleep. The patient reports waking up twice during the night to urinate.
NUTRITION HISTORY:
24 hour recall
7am - tea
8 am - plain rice ( 2 cups)with dhal -340+350(7+21)
1pm - plain rice with dhal
8pm - plain rice with dhal
2370 calories per day
total proteins-84 grams
Menstrual history: menarche at the age of 14 years and has had regular menstrual cycles since then. Marriage at 18 years . pain during periods and passing clots. The menstrual flow lasts for 5 days, with an average of 2 sanitary napkins used per day. Last menstrual period : 12 days ago
OBSTETRIC HISTORY: P2L2 The patient reports having two live births: the first child is a male who is currently 13 years old and the second child is a male who is currently 9 years old. The delivery of the second child was via C-section due to diagnosed as gestational hypertension. The patient received a blood transfusion during the delivery of the second child at 9 months of pregnancy.
FAMILY HISTORY:
Her mother known case of hypothyroidism using 100 micrograms since 10years.
GENERAL EXAMINATION:
After taking consent,patient is examined in well lit room,patient is conscious coherent and cooperative well oriented to time place and person
pallor ++




icterus absent
cyanosis absent
clubbing
lymphadenopathy absent
edema absent
VITALS:
pulse : 83 bpm ,regular rhythm normal volume no radioradial delay no radiofemoral delay BP: 110/80mm hg in right arm examined in sitting position RR: 15 cpm temperature
SYSTEMIC EXAMINATION:
Oral Cavity-Hygiene normal
Teeth: Caries present Tongue: bald Palate / Tonsils / oropharynx - normal INSPECTION:


Shape - round, large with no distention.
Umbilicus - Inverted
Equal symmetrical movements in all the quadrants with respiration.
No visible pulsation,peristalsis, dilated veins and localized swellings.
LSCS Scar present in lower abdomen, hypepigmented.
Hernial orifices are free.
PALPATION : no Local Rise of Temperature
Tenderness present in a left upper quadnant ,left lumbar ,umbilicus and hypogastric regions guarding presnt in left lumbar region.
DEEP :
Enlargement of liver, regular smooth surface , roundededges soft in consistency, tender, moving with respiration non pulsatile
No splenomegaly
PERCUSSION:
Fluid thrill and shifting dullness absent
puddle sign not elicited as patient was not willing
AUSCULTATION
Bowel sounds present.
No bruit or venous hum.
CVS:
Inspection:.
Apical impulse is not observed.
There are no other visible pulsations, dilated and engorged veins, surgical scars or sinuses.
Palpation:
Apex beat was localised in the 5th intercostal space 2cm medial to the mid clavicular line
Position of trachea was central
There we no parasternal heave , thrills, tender points.
Auscultation:
S1 and S2 heard , no murmurs
RESPIRATORY EXAMINATION:
trachea central , no chest wall abnormalities .
bilateral air entry present ,normal vesicular breath sounds.
CNS:
HIGHER MENTAL FUNCTIONS- Normal
Memory intact
CRANIAL NERVES :Normal
SENSORY EXAMINATION
Normal sensations felt in all dermatomes
MOTOR EXAMINATION
Normal tone in upper and lower limb
Normal power in upper and lower limb
Normal gait, slrt bilaterally negative
REFLEXES
Tone- normal
Power- bilaterally 5/5
Reflexes: Right. Left.
Biceps. ++. ++
Triceps. ++. ++
Supinator ++. ++
Knee. ++. ++
Ankle ++. +
CEREBELLAR FUNCTION
Normal function
No meningeal signs were present
Probable diagnosis:
Acute Gastritis with nutritional anemia
INVESTIGATIONS :














IV fluids ns 75ml/hr
INJ pan 40 mg/ IV /od
INJ Zofer 4mg/IV
INJ optineuron 1 amp in 500ml ns/ IV/od
T.PCM 650 mg od
Syp.Sucralfate 10ml/tid
Syp. Cremaffin citrate 15ml
INJ vitkofol 1000mcg/IM/od
T.orofer xt/po/od







IRON PILL induced gastritis
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5412550
Dilutional anemia :
A 55 year old male resident of narketpally mechanic by occupation, came with cheif complaints of abdominal tightness since 1 month, decreased appetite since 1 month
HOPI:
Patient was apparently asymptomatic 1 month back, then he developed abdominal distension which is insidious in onset gradually progressive, fever since 10days high grade associated with chills and rigors and increased on night time relieved by medication
h/o decreased appetite
No h/o pain abdomen ,vomiting, pedal edema ,dyspnea ,jaundice ,cough, hemoptysis,burning micturition
PAST HISTORY:
not a k/c/o dm ,htn,tb, asthma ,epilepsy
PERSONAL HISTORY:
DIET- mixed
APPETITE- decreased
SLEEP- adequate
BOWEL AND BLADDER MOVEMENTS- Regular
ADDICTIONS-
chronic alcoholic drinks 90 ml for 20 years
chronic smoker 9 beedis per days for past 30 years
DAILY ROUTINE 1 month back: patient wakes up at 6 o clock , drinks chai , goes for work , works in a factory ( brick making ) at 1 O clock eats lunch usually rice with curry at 5 o clock comes home watches tv and 8 oclock eats dinner rice with curry and sleeps adequately
present daily routine:
at 6 oclock drinks chai eats 2 idli for breakfast drinks maaza , cannot go to work , appetite decreased .
ON EXAMINATION:
PATIENT IS CONSCIOUS, COHERENT, COOPERATIVE
PALLOR- ABSENT
ICTERUS- ABSENT
CYANOSIS- ABSENT
CLUBBING- ABSENT
LYMPHADENOPATHY- ABSENT
EDEMA- ABSENT








SYSTEMIC EXAMINATION:






























Comments
Post a Comment