1801006072 CASE PRESENTATION
Long Case
Chief complaints
A 50 year old male farmer by occupation came to opd with chief complaints of
1. SOB since 10 days
2.Edema of both upper and lower limb since 6 days
History of presenting illness-
SEQUENCE OF EVENTS
Patient was apparently asymptomatic 14 years ago then he had a history of fall from tree where he got back pain and used medication for that
↓ 8 years ago(2015)
He was diagnosed with diabetes mellitus type 2
↓
2 years ago(2019)- Developed fever cough and loss of appetite diagnosed with TB and took ATT for 6 months
↓
1 year ago - he met with fire accident after that he noticed swelling in legs for which he diagnosed with
ckd
↓
Jan 2023 - In 2023 Jan he developed shortness of breath grade 3
↓
March 2023- 10 days back he had sudden onset of difficulty in breathing which has progressed to
Grade 4 orthopnea present, and Edema of both upper and lower limbs For 6 days
Lower limb edema which is pitting type (grade 4 ) up to the thigh.
In a private hospital And was referred to our hospital for further management.
Past history-
Known case of diabetes mellitus since 8 years and was on medication- metformin
Not a known case of; Hypertension, thyroid, or Asthma.
No history of any surgeries in the past.
Drug history:- intermittent use of NSAIDS for the past 14 years.
Personal history
Mixed diet
Appetite was normal
Bowel and bladder - decreased urinary output since 6 days
Sleep adequate
Addictions
alcohol (daily)stopped 2years ago ,now occasionally
Patient is conscious coherent and cooperative well oriented to time place person
Moderately built and moderately nourished.





Imaginary pillow effect.
Pallor-absent
Icterus-absent
Cyanosis-absent
Clubbing-absent
Lymphadenopathy-absent
Pedal edema- seen bilaterally (pitting type)
Vitals:—
Temperature- afebrile
Pulse rate- 103bpm
RR- 35cpm
Blood pressure-150/90 mmhg
Grbs:- 203mg/dl
SpO2:- 97% @room air
Mild JVP raise is seen
SYSTEMIC EXMINATION-
Cardiovascular system:-
CARDIOVASCULAR SYSTEM:-
INSPECTION:-
Appears normal in shape
Apex beat is not visible
No Dilated veins, scars, sinuses
PALPATION:
1- All inspector findings were confirmed.
2-Trachea is central.
APEX BEAT at 5TH INTERCOSTAL SPACE IN 1 cm LATERAL TO MID CLAVICALE
No palpable murmurs (thrills)
PERCUSSION:-
Heart borders are normal limits.
AUSCULTATION:-
S 1; S 2 heard in ALL THE AREAS
RESPIRATORY SYSTEM:-
INSPECTION:- Chest appears symmetric
No Dilated veins, scars, sinuses
PERCUSSION -

Auscultation:—
NVBS are less heard in infraaxillary,infrascapular and inter scapular regions.
PER ABDOMEN:-
no tenderness
no palpable organs
bowel sounds - present
CNS EXAMINATION:-
The patient is conscious.
No focal deformities.
cranial nerves - intact
sensory system - intact
motor system - intact
INVESTIGATIONS:-
7/3/ 23:-
HAEMOGLOBIN %- 10.0 gms %
PCV :- 31.8 vol%
8/3/23:-
HAEMOGLOBIN - 11.3 gms %
PCV :- 36.1 vol%
9/3/23:-
HAEMOGLOBIN %- 11.0 gms %
PCV - 34.5 vol%
SERUM CREATININE - 5.6 mg/dl.
10 /3/23 :-
ULTRASOUND:-
IMPRESSION:- B/L GRADE IN RENAL PARENCHYMAL CHANGES
B/L MODERATE PLEURAL EFFUSIONS
MILD ASCITES
SERUM CREATININE
5.9 mg/dl
SERUM POTASSIUM
3.4 mEq/L
HAEMOGLOBIN % - 10.6 gm
PACKED CELL VOLUME:- 34.2 vol% ( decreased)
11/3/23:-
SERUM CREATININE:- 5.9 mg/dL
Then referred to our hospital
13/3/23 :-
Serology:
HIV: NEGATIVE
Anti-HCV antibodies:- NON-REACTIVE
HbsAg:- NEGATIVE
RANDOM BLOOD SUGAR: 125mg/dl
CUE:- NORMAL
S.UREA: 64mg/dl (N:- 12-42mg/dl)
S. CREATININE: 4.3 mg/dl
S. Na+: 138
S. K+: 3.4 (3.5-5.5)
S. Cl-: 104
CBP:-
Hb:- 12.6 gm/dl
HbA1C: 6.5%
FASTING BLOOD SUGAR:- 93 mg/dl
POST-LUNCH BLOOD SUGAR:- 152 mg/dl
Liver function tests:-
Total bilirubin-0.9mg/dl
Direct bilirubin-0-1mg/dl
Indirect bilirubin-0.8mg/dl
Alkaline phosphatase- 221 u/l
AST-40u/L
ALP- 81u/L
Chest X-ray


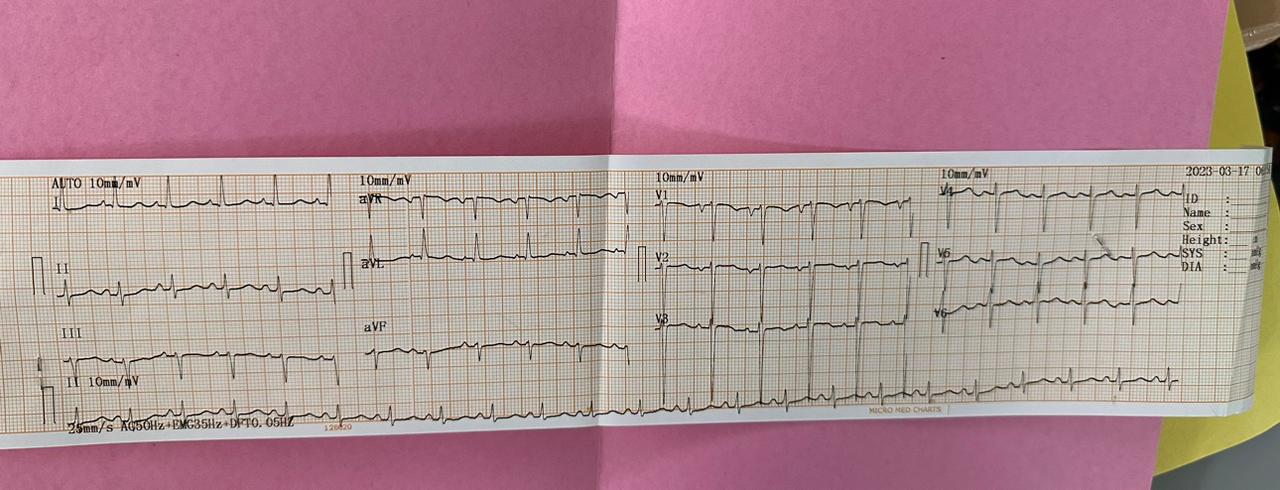
ECG
USG CHEST:
IMPRESSION:
BILATERAL PLEURAL EFFUSION (RIGHT MORE THAN LEFT) WITH UNDERLYING COLLAPSE.
USG ABDOMEN AND PELVIS:
MILD TO MODERATE ASCITES
RAISED ECHOGENICITY OF BILATERAL KIDNEYS
2D echo:-
Mild LV dysfunction-present
MR +ve, TR +ve (moderate)
Provisional diagnosis:-
-Heart failure with mid range ejection fraction
With Acute kidney injury on chronic kidney disease (NSAID induced or diabetes induced).
With old pulmonary kochs (2 yrs ago)
And bilateral pleural effusion (left side is more than right side)
Treatment:—
-Fluid restriction less than 1.5lts per day.
-salt restriction less than 1.2gm perday
-INJ Lasix 40 mg IV/BD.
-TAB MET XL 25mg PO/OD
-TAB Cinod 5 mg PO/OD.
-INJ human actrapid insulin SC/TID
-INJ PAN 40 mg IV/OD
-INJ ZOFER 4mg IV
- vitals monitoring
-TAB Ecosprin AV 75/10 mg PO/HS.
---------------------------------------------------------------------------------------------------------------
short case
CHIEF COMPLIANTS
A 64 year male patient presented with cheif compliants of:
Cough since 10 days
Loose stools since 10 days
Hiccups since 7 days
Inability to speak since 4 days
fever 4 days back
loss of appetite since 3 days
HISTORY OF PRESENT ILLNESS
patient was apparently asymptomatic 10 days back then he developed diarrhoea -5 episodes/day for 1 day which relieved on medication.Then he developed having hiccups since 7 days and anorexia for 3days.since 25/12/22 he is unable to talk.

PAST HISTORY
h/o panic attack one month back secondary to family issues
-DM2 since 6 yrs ,
on medication :tab Metformin OD , tab Glimiperide OD
-NO HISTORY OF HTN, TB, Asthma, epilepsy, CAD, CVD
Personal History :-
Appetite - reduced
Diet - Mixed
Sleep - adequate
Bowel and bladder movements - incontinence
Addictions: Occasional alcoholic ( during functions ) ,chews tobacco daily
Allergies : No allergies
Family history:
Mother is a known case of TB 5years back who is treated adequately.
GENERAL EXAMINATION
Patient is unconscious ,incoherent , uncooperative
Moderately Built and Moderately Nourished .
Pallor : present
Icterus : absent
Cyanosis: absent
Clubbing : absent
Lymphadenopathy : absent
Edema : absent
Vitals :-
Temp: Afebrile
BP : 100 / 50 mmHg
PR : 120 bpm
RR : 16 cpm
SPO2 : 98 % at RA
GRBS : 193 mg/dl
Fever

SYSTEMIC EXAMINATION:
CNS examination :-
HIGHER MENTAL FUNCTIONS
State of consciousness : unconscious
Speech : incoherent
Sensory system :-
Pain - Normal
Temp - normal
Cranial nerves :
Not elicited patient not cooperative
CNS
Reflexes :-
Biceps + +
Tricep s + +
Supinator + +
Knee +
Ankle. ++
Flexor. Plantar. Plantar
Finger nose in coordination - no
Heel knee in coordination - no
CVS : S1 S2 + ,no murmurs ,no thrills
Respiratory System : decreased air entry on left side . Crackle sound are heard. Position of trachea - central.
Per abdominal examination:-
Soft , non tender , no signs of organomegaly


Chest X-ray

INVESTIGATIONS:
CSF ANALYSIS
Sugar 51 mg/dl (normal 60-90mg/dl)
Protein 203mg/dl( normal 10- 45mg/dl)
Chloride 121 mmol/L (116-127mmol/l)
CSF CELL COUNT
Colour - colour less
Appearance - slightly cloudy
Total cells - 90 cells /cumm
Lymphocytes -60%
Neutrophils - 40%
COMPLETE URINE EXAMINATION
Colour - pale yellow
Appearance - clear
Reaction - acidic
Specific gravity - 1.010
Albumin -nil
Sugar -nil
Bile salts - nil
Bile pigments- nil
Pus cells - 2-3cells(normal 0-5/HPF)
Epithelial cells- 2-3 cells(normal 0-5HPF)
RBC -nil (normal 0-5/HPF)
Crystals-nil
Casts-nil
Amorphous deposits-absent
BLOOD UREA -124mg/dl(normal 17-50mg/dl)
APTT
APTT TEST- 31sec(normal 24- 33sec)
Bleeding and clotting time
Bleeding time- 2min 30sec(normal2 -7 min)
Clotting time- 5min (normal 1- 9min)
PROTHROMBIN TIME - 15sec ( normal 10 -16 sec)
MRI BRAIN PLAIN
DIFFUSE CEREBRAL ATROPHY
BLOOD SUGAR 159mg/dl
DIAGNOSIS
Altered sensorium secondary to tuberculous
meningitis
Management:-
1) IVF 0.9 %NS IV @ 50 ml / hr
2) Inj , 1 amp Optineuron in 500 ml NS IV /OD
3) tab Ecosprin AV 75/10 RT / OD / HS
4) GRBS monitoring 6 th hrly
5) Inj Thiamine 200 mg IV/BD in 100 ml NS



Comments
Post a Comment