1801006075 CASE PRESENTATION
LONG CASE
48 yr old male daily wage labourer resident of xxx was brought to medicine opd with chief complaints of
Shortness of breath since 5 days.
Decreased urinary output since 5 days.
And swelling of both the lower limbs since 1 yr which is on and off.
HISTORY OF PRESENT ILLNESS-
Patient was apparently asymptomatic 1 yr back then he developed bilateral pedal edema which was (on and off since 1 yr) and was present from ankle to knee pitting type .For this he went to hospital and there he was put on conservative management and on routine examination was diagnosed with hypertension and was started on anti-hypertensive drugs(telmisartan - 40 mg OD).
On sunday night (12/03) night around 12 AM he had an episode of shortness breath ( Class 4 - NYHA) which was sudden and associated with paroxysmal nocturnal dyspnea and orthopnea
No history of any chest pain or sweating or palpitations.
There was decreased urine output ,narrow streamlined.
And no history of any burning micturition or fever.
There is no history of cough
Stay in hospital-
He has undergone dialysis 3 times since his admission
PAST HISTORY-
History of NSAIDS abuse 4 yrs back used due to diffuse chronic bone pain.
Known case of hypertension since 1 yr using ( Telmisartan 40 mg)
Not a known case of diabetes , asthma, epilepsy, tuberculosis.
No similar complaints in the past.
FAMILY HISTORY-
No significant family history.
PERSONAL HISTORY-
Daily Routine-
He wakes around 6 AM and get ready to go to work and works for around 5-6 hours and comes back home have rest, he has his regular meals at 8AM ,1 PM and 8 PM and retires for the day around 10PM.
He is no more working
Diet - Mixed
Appetite - Normal
Bowel and bladder movements- Regular but decreased micturation.
Addictions - Smoking beedi (4 beedis per day so 6 pack years) and alcohol since 25 years ocassionally.
GENERAL EXAMINAT-
Consent was taken.
Patient was examined in a well lit room with adequate ventilation with a attendant present.
Patient is conscious coherent and cooperative well oriented to time place and person moderate built and nourished.
Pallor - Present


Icterus - Absent
Cyanosis - Absent
Clubbing - Absent
Lymphadenopathy - Absent
Edema - b/l lower limbs pitting type extending beyond ankle.

Vitals-
Temperature - 98.6 F
Pulse Rate - 74 beats per minute
Blood Pressure - 130/80 mm Hg
Respiratory Rate - 16 cycles per minute
Spo2 - 95%
CLINICAL PICTURES-




SYSTEMIC EXAMINATION-
CVS -
Inspection-
No rise in JVP
No precordial bulge
No visible pulsations
No chest wall defects
Palpation-
Apical impulse - Diffuse in anterior axillary line at 6th intercostal space
No parasternal heaves and thrills
Auscultation-
S1 and S2 heard
RESPIRATORY SYSTEM-
Inspection-
Trachea is in midline
Presence of an healing crusted ulcer in right hemithorax medial to right nipple.

No other scars and sinuses.
Shape is elliptical
Chest is bilateral symmetrical
Bilateral air entry present
No chest and spinal deformities
Palpation-
Trachea is in midline
Symmetrical chest expansion
Chest circumference- 34 inches
No tenderness over chest
Percussion-
Left. Right
Supraclavicular. R. R
Infraclavicular. R. R
Mammary. R. R
Inframammary. R. R
Axillary. R. R
Infraaxillary. R. R
Suprascapular. R. R
Infrascapular. R. R
Inter scapular. R. R
(R - resonanat)
Auscultation-
Lt. Rt
Supraclavicualr. Nvbs. Nvbs
Infraclavicular. Nvbs. Nvbs
Mammary. Nvbs. Nvbs
Inframammary. Wheeze. Nvbs
Axillary. Nvbs. Nvbs
Infraaxillary Wheeze. Nvbs
Suprascapular. Nvbs. Nvbs
Infrascapular. Nvbs. Nvbs
Interscapular. Nvbs. Nvbs
(Nvbs - non vesicualr breath sounds)
Abdominal examination-
Inspection-
Shape of abdomen is scaphoid
Umbilicus inverted
No visble pulsations peristalsis or dilated veins
Free hernial orifces
Palpation -
No local rise in temperature
No tenderness present
No palpable mass
Auscultation-
Bowel sounds heard
Central nervous system examination-
Speech normal
Intact higher mental functions
Cranial nerve examination - N
Motor examination -
Normal tone
Power 5/5 in both upper and lower limbs
Intact reflxes
Sensory examination -
Normal
Provisional diagnosis-
Heart failure with hypertension
Chronic kidney disease.
Investigations-
Hemogram -
16/03 -
Hemoglobin - 7.7 gm/dl (13-17 gm/dl)
Total count - 14,100 cells/cumm(4000-10000 cells/cumm)
Lymphocytes - 16% (20-40%)
PCV - 23.1 vol% (40-50 vol%)
SMEAR :
RBC - Normocytic normochromic
WBC - increased count
Platelets - adequate
CUE-
Serum creatinine - 4.0 mg/dl (0.9 -1.3 mg/dl)
Blood urea - 95mg/dl (12-42 mg/dl)
E Gfr - 18 ( >65)
ABG :
PH 7.43 (7.35-7.45)
Pco2 - 31.6 mmHg (35-45 mmhg)
Po2 - 64.0 mmHg(85-95 mmhg)
HCO3 - 21.1 mmol/l
Urine examination :
albumin ++
sugar nil
pus cells 2-3
epithelial cells 2-3
Red blood cells 4-5
Random blood sugar - 124 mg/dl
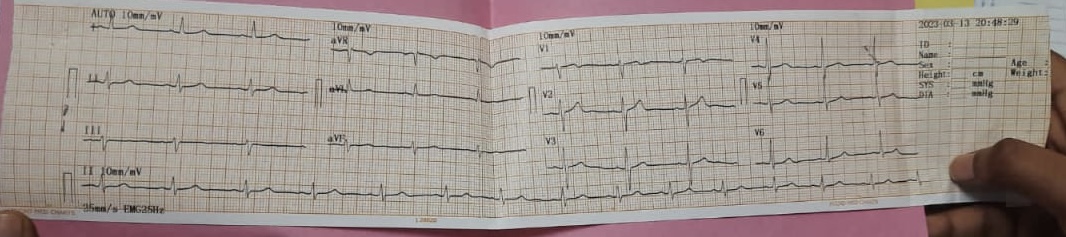
ECG-

X-RAY -
13/03-

2 D echo -
Final Diagnosis -
Heart failure secondary to chronic kidney disease (due to NSAIDS abuse)
Treatment -
Ryle’s feed : 100 ml milk with 2 scoops protein powder 4th hourly and 100 ml water 6th hourly.
Inj. Thiamine 100mg in 50 ml NS TID
Inj. Piptaz 2.25g IV TID
Inj. LASIX 40mg IV BD
Inj. Erythropoietin 4000IU SC Once weekly
Inj. PAN 40 mg IV OD
Tab. Nicardia Retard 10mg RT BD
Tab. Metoprolol 12.5mg RT OD
Tab. NODOSIS 500 mg RT BD
Tab. Orofer RT OD
Cap. BIO D3 RT OD
Hemodialysis
Nebulisation with Duolin 8th hourly and Budecort 12th hourly
Intermittent CPAP
Allow sips of oral fluid
Monitor vitals
----------------------------------------------------------------------------------------------------------------------------------------------------
SHORT CASE
A 30 yr old female resident of xxx farmer by occupation presented to the OPD with chief complaints of generalised weakness since last month , stomach pain from last 4 days and vomiting from the last 2-3 days.
HISTORY OF PRESENTING ILLNESS-
Patient was apparently asymptomatic 1 month ago then she developed fever which was sudden in onset and intermittent and was relived on medication(PCM) not associated with chills and rigirs she also had vomiting which was non blood stained bilious and projectile 2-3 times a day and small volume watery diarrhoea which was non blood stained for 10 days. At that time the patient came to our hospital and diagnosed as acute gastritis and on investigation incidentally found to be having an low heamoglobin of 5g/dl . She was not admitted due to personal reasons and was prescribed oral iron medications.

Then few days later she had stomach pain which was diffuse throbbing and intermittent and had no aggravating or relieving factors and also had vomiting which was non projectile occurs after meals non blood stained and bilious and contians digested food as its particles. So she was presented to our hospital on 13/03/2023.
There is history of shortness of breath present 1 month back which was insidious and gradually progressed to class 3 (NYHA classification) and is resolved now.
There is no history of weight loss ,orthopnea, paroxsymal nocturnal dyspnea or any bleeding manifestations.
Daily Routine-
She wakes up early around 6-6:30 AM and freshen ups has tea in morning and does all household work and eats rice mainly in her all meals. She is presently not working due to non - farming season.
NUTRITION RECALL 24 Hrs-
7 AM - Tea (105 cal)
8 AM - Rice(2 cups - 427 cal) dal (198 cal)
2 PM - Rice dal
8 PM - Rice dal
10 PM - Milk(149 cal)
Total calories 2129 calories per day
PAST HISTORY-
Not a known case of DM/HTN/Aastham/Epilepsy/Tuberculosis/Leprosy/CKD/CAD
PERSONAL HISTORY-
Diet - Mixed
Appetite - Normal
Bladder movements- Regular
Bowel movements- Regular
Sleep - Adequate
Allergy - No
Addictions - No
MENSTRUAL HISTORY-
Age of menarche - 14 yrs
Cycles regular 4 day flow with 40 days duration associated with pain and clots
Uses 2 sanitary napkins/day.
Last menstrual period was on 5/3/23.
MARITAL HISTORY-
Marital life - 15 yrs
P2L2
1st child - 2 yrs after marriage male child (13 yrs old) healthy by LSCS.
No usage of any contraception
Concieved after 4 yrs.
During 2nd child pregnancy-
History of parentral iron in the 8th month of pregnancy
History of blood transfusions in the 9th month of pregnancy.
2nd child - Lscs male (9 yrs old ) healthy.
Then tubectomy was done.
FAMILY HISTORY -
Mother is a known case of hypothyroidism and on medication since 10 yrs.
GENERAL EXAMINATION-
Consent is taken and patient us examined in a well lit room with adequate ventilation with a female attendant and she is conscious coherent and co operative well oriented to time place and person.
Pallor - Present



Icterus - Absent
Cyanosis - Absent
Clubbing - Absent

Lymphadenopathy - Absent
Pedal Edmea - Absent

VITALS -
Pulse Rate - 67 beats per minute which is regualr in rhythm normal volume and there is no radioradial and radiofemoral delay
Blood Pressure - 110/80 mm Hg in right arm sitting position
Respiratory Rate - 14 counts per minute
Temperature - 38.8 C
SYSTEMIC EXAMINATION-
Abdomen Examination-
Inspection -


Shape - Round with no distension
Umbilicus - Inverted
LSCS scar in lower abdomen
No visible discharging sinuses ,swellings ,dilated veins , peristalsis or pulsations .
Hernial orifices are free.
Palpation -
No local rise of temperature
Tenderness present which is diffuse over left upper quadrant, left lumbar, umbilicus and hypogastric regions.
No hepatomegaly
No splenomegaly
PERCUSSION-
Fluid thrill and shifting dullness absent.
Auscultation-
Bowel sounds present
CVS -
Inspection-
No visible apical impulse
No other sinuses scars or dilated veins and pulsations.
Palpation-
Apex beat was localized in the 5 th ICS 2cm medial to mid claviclular line
No thrills or parasternal heaves.
Auscultation-
S1 and S2 heard
No murmurs
Respiratory Examination-
Inspection-
Chest appears bilaterally symmetrical
Respiratory movements appear equal on both sides
Trachea central in position
Palpation-
Trachea is central
Auscultation-
B/l air entry
Non vesicular breath sounds
CNS-
Higher Mental Functions - Normal
Memory- Intact
Cranial Nerve Examination- Normal
Motor Examination-
Normal tone and power in both upper and lower limbs(5/5)
Reflexes -
Superficial- Corneal conjuctival and plantar reflexes present on both sides
Deep -
Rt Lt
Biceps 2+ 2+
Triceps 2+ 2+
Knee 3+ 3+
Ankle 1+ 1+
Sensory Examination -
Fine touch vibration and joint sense is intact on both sides.
Pain and temperature intact on both sides
Cerbellar functions - Normal
No signs of meningeal irritation.
PROVISIONAL DIAGNOSIS-
Acute gastritis and anemia.
INVESTIGATIONS-
Hemogram -
Day 1 - 13/3 -
Hemoglobin levels - 10.5 gm/dl (12-15 gm/dl)
Total WBC count - 13,400 ( 4000- 10000)
MCV - 72.7 (83-101)
MCH - 19 (27-32)
MCHC - 27.2 (31.5 - 34.5)
RBC count -
Perioheral smear - Microcytic hypochromic anemia with few normocytes microcytes macrocytes and pencil cells and leucocytosis.
Day 2 - 14/3 -
Hemoglobin levels - 9.1 (12-15)
PCV - 33.6 (35-46)
MCV - 72.9 (83-100)
MCH - 19.7 (27-32)
MCHC - 27.1 (31.5 - 34.6)
Day 3 - 15/3-
Hemoglobin- 8.8 (12-15)
PCV - 32.4 (36-46)
MCV - 75.2 (83-101)
MCH - 20.4 (27-32)
MCHC - 27.2 (31.5 - 34.5)
Electrolytes-
Day 1 - 13/3
Pottasium - 5.4 mEq/L ( 3.5 - 4.5)
Sodium chloride and calcium normal levels
Day 2 - 14/3
Pottasium - 4.1 ( in normal range 3.5-4.5)
Serum creatinine - 0.6 mg/dl (0.6 -1.1)
Blood urea - 26 mg/dl (12-42)
Retic count - 1.5%
Serum iron - 38 microg/dl (37-145)
ECG -
USG -
Right small kidney - 5.6*2.9cm
Left kidney - 10.5*4.8 cm
Final diagnosis-
Dimorphic anemia and acute gastritis (resolved )
Plan of care -
IV fluids NS 75 ml/hr
Inj pan 40mg/IV/OD
Inj zofer 4mg/IV
Inj optineuron 1amp in 500 ml NS/IV/OD
Tab PCM 650 mg OD
Syp sucralfate 10 ml/TID
Syp cremaffin citrate 15 ml
Inj vitkofol 1000 microgram/IM/OD
Tab orofer






Comments
Post a Comment