1801006131 CASE PRESENTATION
long case
Chief complaints:
A 55 year old male came with c/o slurring of speech since 2 days
C/o deviation of mouth towards left side since 2 days
History of present illness :
Patient was apparently alright 2 days back then he had slurring of speech which is sudden in onset and Patient’s wife noticed deviation of mouth towards left side on the same day
No weakness of upper and lower limb.
No h/o trauma
No h/o involuntary movenents
No h/o of numbness or paresthesia
No LOC/ altered sensorium.
No h/o altered smell
No h/o blurring of vision
No drooling of sliva
No drooping of eyelids
No difficulty in swallowing
Past history:
K/c/o HTN since 1 year on ATENOLOL and AMLODIPINE 5mg
He is not a k/c/o DM II, CVA, CAD, ASTMHA
GENERAL EXAMINATION:
Patient is conscious coherent cooperative
No pallor, icterus, cyanosis, clubbing, generalised edema or lymphadenopathy
Vitals :
bp-130/80
Pr -90bpm
RR: 18
Spo2 -98% @ RA
Systemic examination:
CNS:
Higher mental functions
conscious,coherent and cooperative
memory- intact
Speech - comprehension present, no fluency, repetition present
Cranial nerve examination
I- Olfactory nerve- sense of smell present
II- Optic nerve- direct and indirect light reflex present
III- Oculomotor nerve, IV- Trochlear and VI- Abducens- no diplopia, nystagmus or ptosis
V- Trigeminal nerve- Masseter, temporalis and pterygoid muscles are normal. Corneal reflex is present.
VII- Facial nerve- face is symmetrical, forehead wrinkling present , nasolabial folds prominent on both sides.
VIII- Vestibulocochlear nerve- decreased hearing of the left ear ( rinner’s negative for 256 Hz and 512 Hz) and normal hearing of the right ear
IX- Glossopharyngeal nerve- palatal movements present and equal
X- Vagus- palatal movements present and equal
XI- Accessory nerve- sternocleidomastoid contraction present
XII- Hypoglossal nerve- deviation of tongue to right side and no fasciculations present
Sensory system examination:



Flexion
Gait
CVS: S1 & S2 heard. No murmurs
Respiratory system:Normal vesicular breath sounds heard
Abdomen: Soft and non-tender.No organomegaly


Investigations:
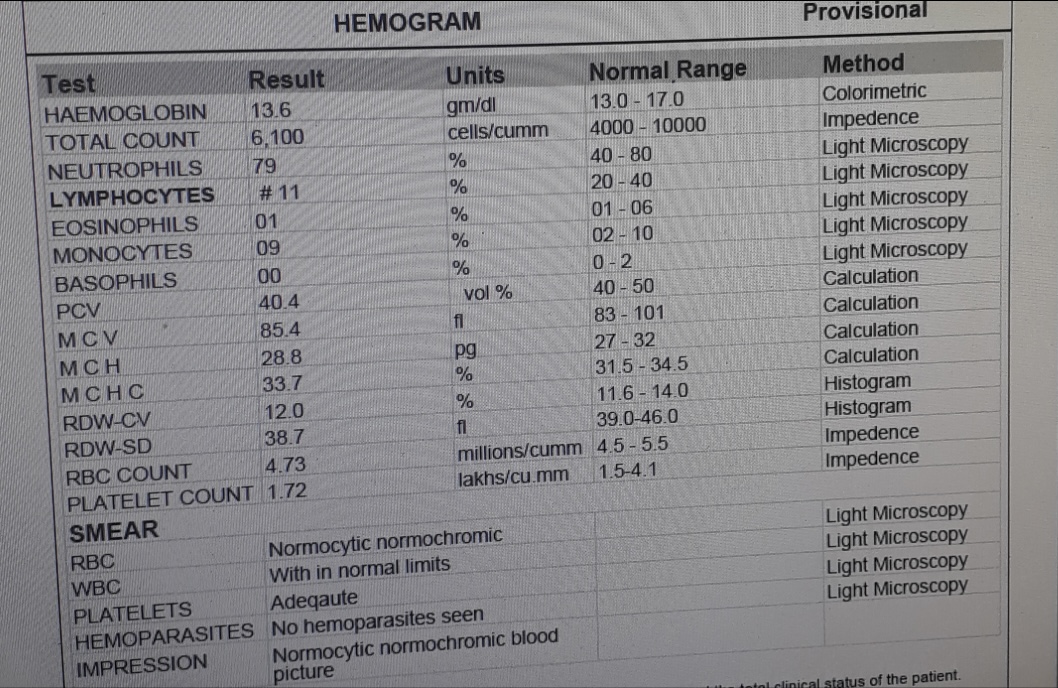
Complete blood picture
Haemoglobin:11.7
Peripheral smear: normocytic normochromic anemia
Red blood cells:3.86
Pcv:34.6
Platelet count:2.10
Total leucocyte count:5,100
Fasting blood sugar : 92 mg/dl
Serum creatinine :1.3 mg/dl
Blood urea 38 mg/dl
CUE:
Colour : pale yellow
Appearance : clear
Reaction :acidic
Albumin:nil
Sugar: nil
Bile salts and bile pigments : nil
RBC : nil
Crystals :nil
Casts : nil
pus cells:2-3
epithelial cells-2-3
Serum electrolytes
Sodium: 145 mEq/L
Potassium:4.2mEq/L
Chloride:104 mEq/L
Calcium ionized:1.11 mmol/L
ECG:

MRI :







Provisional diagnosis:
INJ. OPTINEURON 1 AMP IN 500ML
NS IV OD
TAB. CLOPITAB 75 MG PO/OD
TAB. ECOSPRIN AV 75/10 PO
----------------------------------------------------------------------------------------------------------------------------------------------------
short case
40year old male who is a farmer by occupation and came to opd with
CHIEF COMPLAINTS;
loose stools yesterday 2 a.m
vomiting since today morning
HISTORY OF PRESENT ILLNESS;
Patient was apparently asymptomatic till yesterday evening then
he suddenly developed loose stools yesterday night @ 2 a.m 40 to 50 episodes of loose stools,large quantity, white coloured stools,foul smelling, non blood tinged
c/o vomiting 3 episodes in the morning, food particles as content,non projectile, non bilious, non foul smelling relieved on their own.for loose stools they went to local RMP and got symptomatic treatment
similar episodes of vomiting and loose stools 10 years back and got admitted for 1 week and discharged
H/O insecticides spray yesterday morning
No H/O outside food and water intake .No similar complaints to his family,neighbours
No h/o fever,cough,cold
PAST HISTORY;
N/k/c/o DM,HTN,TB,EPILEPSY, CVA,CAD,THYROID DISORDERS
FAMILY HISTORY:-
insignificant
PERSONAL HISTORY:-
DIET-mixed
APEPTITE- decreased
BOWEL &BLADDER-Increased,increased burning micturition since today
SLEEP-Adequate.
ADDICTIONS- No
GENERAL EXAMINATION:-
Patient is conscious , coherent,cooperative.
Well oriented to time place & person
Moderate built and moderately nourished.
Pallor absent
No cyanosis, clubbing, icterus, LN
Vitals :
Bp -140/100 mmhg
PR -96 bpm ;
RR : 22cpm
Spo2 : 96 on RA
GRBS:128 mg/dl
CENTRAL NERVOUS SYSTEM;
patient is conscious
speech is normal
no signs of meningeal irritation
Sensory examination: Normal
reflexes;
RIGHT LEFT
BICEPS +2 +2
TRICEPS +2 +2
SUPINATOR +1 +1
KNEE +2 +2
ANKLE +2 +2
Rhomberg's negative
Cerebellum:
Nystagmus-absent
Tremors- absent
Finger nose test- normal
Dysdiadokinesia- absent
CARDIOVASCULAR SYSTEM:-
S1 S2 heard
No murmurs.
RESPIRATORY SYSTEM:-
Dyspnea-absent
No wheeze
Breath sounds - vesicular
No Adventitious sounds
ABDOMINAL EXAMINATION:-
No tenderness
No palpable liver and spleen.
Bowel sounds - PRESENT
Investigation:








USG :

ECG :

X-ray

2D-Echo




Comments
Post a Comment